Lee Seungyup, Sahadevan Jayakumar, Khrestian Celeen M, Cakulev Ivan, Markowitz Alan, Waldo Albert L
From Departments of Medicine and Surgery, Case Western Reserve University (S.L., J.S., C.M.K., I.C., A.L.W.); Division of Cardiovascular Medicine, Case Western Reserve University (J.S., I.C., A.L.W.); and Valve Center, Harrington Heart and Vascular Institute, University Hospitals Case Medical Center; Cleveland, OH (A.M.).
Circulation. 2015 Dec 1;132(22):2108-17. doi: 10.1161/CIRCULATIONAHA.115.017007. Epub 2015 Oct 23.
The mechanism(s) of persistent and long-standing persistent (LSP) atrial fibrillation (AF) is/are poorly understood. We performed high-density, simultaneous, biatrial, epicardial mapping of persistent and LSP AF in patients undergoing open heart surgery (1) to test the hypothesis that persistent and LSP AF are due to ≥ 1 drivers, either focal or reentrant, and (2) to characterize associated atrial activation.
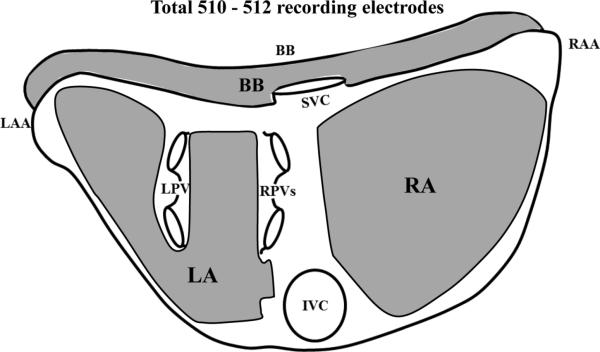
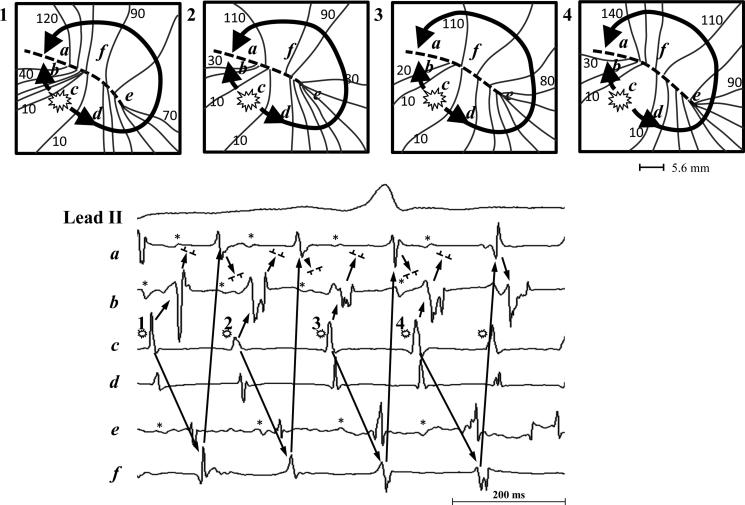
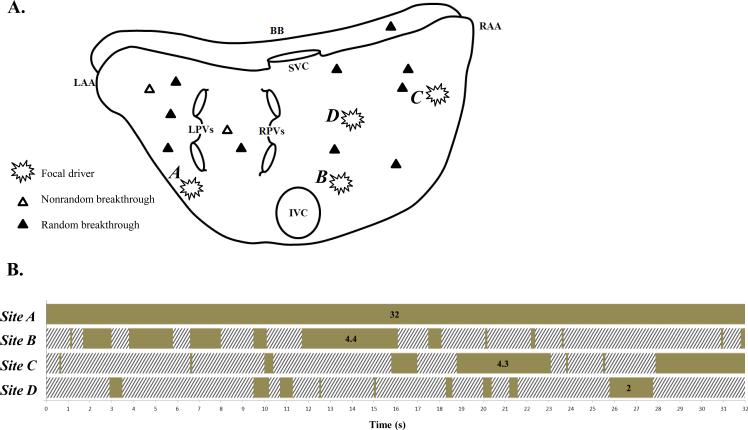
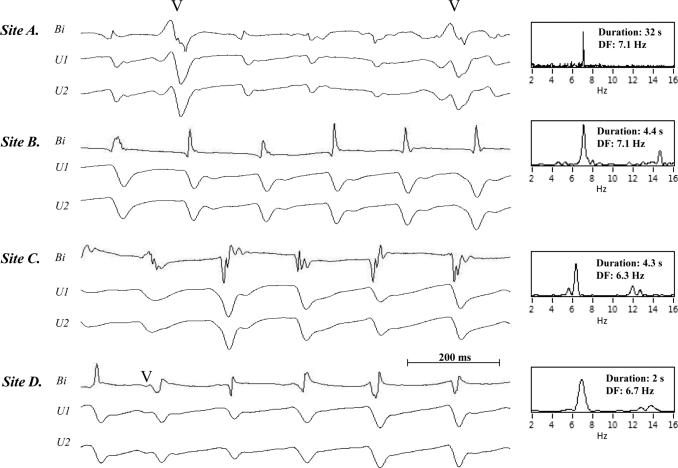
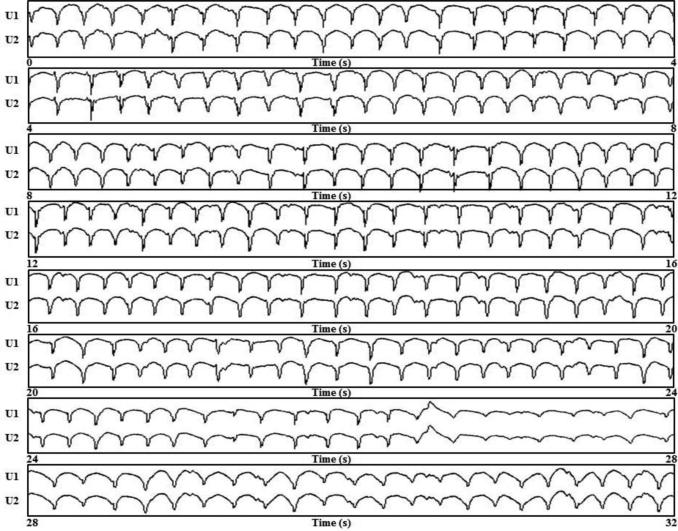
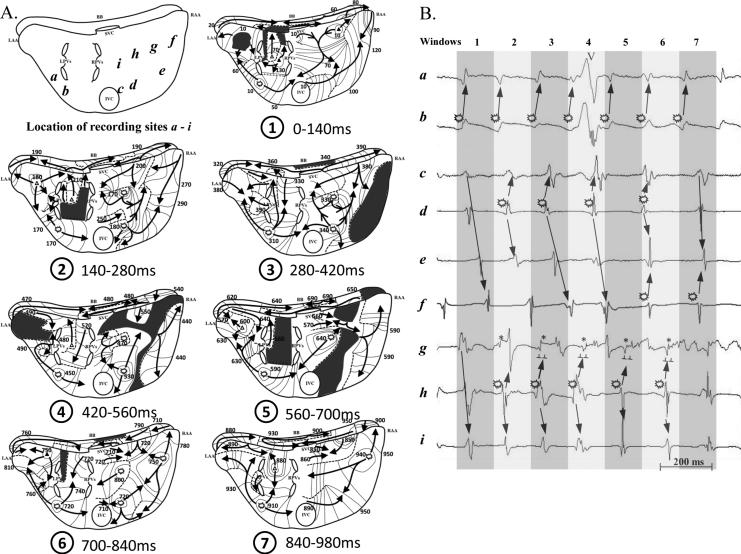
Twelve patients with persistent and LSP AF (1 month to 9 years duration) were studied at open heart surgery. During AF, electrograms were recorded from both atria simultaneously for 1 to 5 minutes from 510 to 512 epicardial electrodes with ECG lead II. Thirty-two consecutive seconds of activation sequence maps were produced per patient. During AF, multiple foci (QS unipolar atrial electrograms) of different cycle lengths (mean, 175 ± 18 ms) were present in both atria in 11 of 12 patients. Foci (2-4 per patient, duration 5-32 s) were either sustained or intermittent, were predominantly found in the lateral left atrial free wall, and likely acted as drivers. Random and nonrandom breakthrough activation sites (initial r or R in unipolar atrial electrograms) were also found. In 1 of 12 patients, only breakthrough sites were found. All wave fronts emanated from foci and breakthrough sites, and largely either collided or merged with each other at variable sites. Repetitive focal QS activation occasionally generated repetitive wannabe reentrant activation in 5 of 12 patients. No actual reentry was found.
During persistent and LSP AF in 12 patients, wave fronts emanating from foci and breakthrough sites maintained AF. No reentry was demonstrated.
持续性和长期持续性(LSP)心房颤动(AF)的机制尚未完全明确。我们对接受心脏直视手术的患者进行了持续性和LSP AF的高密度、同步双心房心外膜标测,(1)以检验持续性和LSP AF是由≥1个驱动因素(局灶性或折返性)引起的这一假设,(2)并对相关的心房激动进行特征描述。
对12例持续性和LSP AF患者(病程1个月至9年)在心脏直视手术期间进行了研究。在房颤期间,通过心电图II导联,从510至512个心外膜电极同时记录双心房电图1至5分钟。每位患者生成32秒连续的激动序列图。在房颤期间,12例患者中有11例双心房均存在多个不同周期长度(平均175±18毫秒)的局灶(QS单极心房电图)。局灶(每位患者2 - 4个,持续时间5 - 32秒)持续或间歇出现,主要位于左心房外侧游离壁,可能起驱动作用。还发现了随机和非随机的突破激动部位(单极心房电图中最初的r或R)。12例患者中有1例仅发现了突破部位。所有波前均发自局灶和突破部位,并且在不同部位大多相互碰撞或融合。12例患者中有5例,重复性局灶QS激动偶尔会产生重复性的拟折返激动。未发现实际的折返。
在12例患者的持续性和LSP AF期间,发自局灶和突破部位的波前维持了房颤。未证实有折返。