Preston Ioana R, Roberts Kari E, Miller Dave P, Sen Ginny P, Selej Mona, Benton Wade W, Hill Nicholas S, Farber Harrison W
From Tufts University School of Medicine, Boston, MA (I.R.P., K.E.R., N.S.H.); ICON Clinical Research, San Francisco, CA (D.P.M., G.P.S.); Actelion Pharmaceuticals US Inc., South San Francisco, CA (M.S., W.W.B.); and Boston University School of Medicine, Boston, MA (H.W.F.).
Circulation. 2015 Dec 22;132(25):2403-11. doi: 10.1161/CIRCULATIONAHA.115.018435. Epub 2015 Oct 28.
Long-term anticoagulation is recommended in idiopathic pulmonary arterial hypertension (IPAH). In contrast, limited data support anticoagulation in pulmonary arterial hypertension (PAH) associated with systemic sclerosis (SSc-PAH). We assessed the effect of warfarin anticoagulation on survival in IPAH and SSc-PAH patients enrolled in Registry to Evaluate Early and Long-term PAH Disease Management (REVEAL), a longitudinal registry of group I PAH.
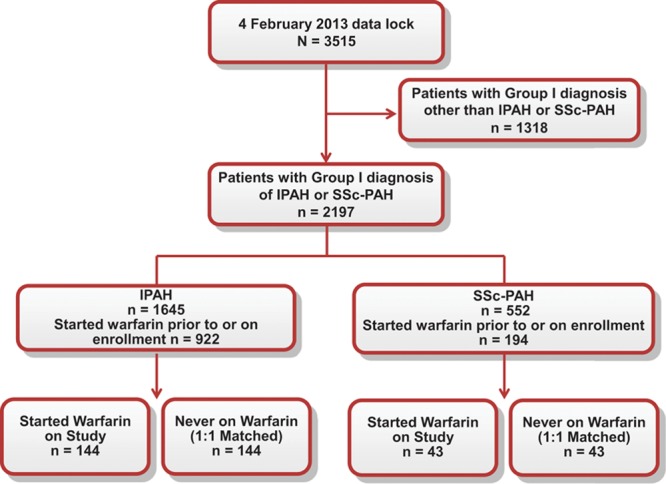
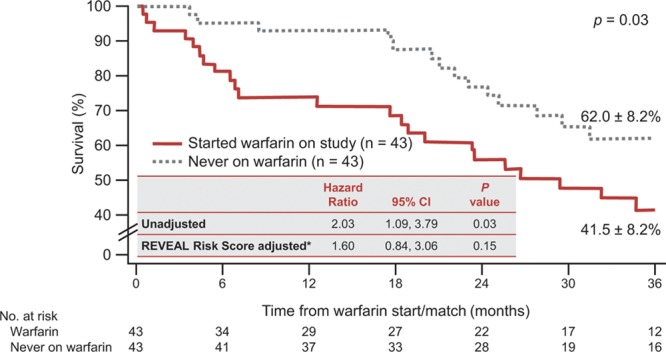
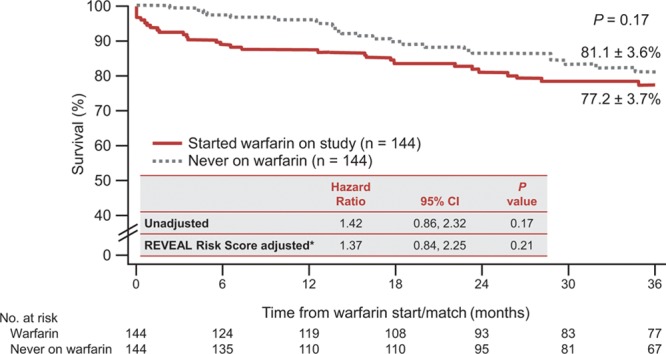
Patients who initiated warfarin on study (n=187) were matched 1:1 with patients never on warfarin, by enrollment site, etiology, and diagnosis status. Descriptive analyses were conducted to compare warfarin users and nonusers by etiology. Survival analyses with and without risk adjustment were performed from the time of warfarin initiation or a corresponding quarterly update in matched pairs to avoid immortal time bias. Time-varying covariate models were used as sensitivity analyses. Mean warfarin treatment was 1 year; mean international normalized ratios were 1.9 (IPAH) and 2.0 (SSc-PAH). Two-thirds of patients initiating warfarin discontinued treatment before the last study assessment. There was no survival difference with warfarin in IPAH patients (adjusted hazard ratio, 1.37; P=0.21) or in SSc-PAH patients (adjusted hazard ratio, 1.60; P=0.15) in comparison with matched controls. However, SSc-PAH patients receiving warfarin within the previous year (hazard ratio, 1.57; P=0.031) or any time postbaseline (hazard ratio, 1.49; P=0.046) had increased mortality in comparison with warfarin-naïve patients.
No significant survival advantage was observed in IPAH patients who started warfarin. In SSc-PAH patients, long-term warfarin was associated with poorer survival than in patients not receiving warfarin, even after adjusting for confounders.
URL: http://www.clinicaltrials.gov. Unique identifier: NCT00370214.
特发性肺动脉高压(IPAH)患者推荐长期抗凝治疗。相比之下,关于系统性硬化症相关肺动脉高压(SSc-PAH)患者抗凝治疗的数据有限。我们评估了华法林抗凝治疗对参与“评估肺动脉高压疾病早期和长期管理注册研究(REVEAL)”的IPAH和SSc-PAH患者生存的影响,REVEAL是一项关于I组肺动脉高压的纵向注册研究。
在研究中开始使用华法林的患者(n = 187),按入组地点、病因和诊断状态与从未使用过华法林的患者进行1:1匹配。进行描述性分析以比较不同病因的华法林使用者和非使用者。从华法林开始使用时间或匹配对中的相应季度更新时间开始进行有和没有风险调整的生存分析,以避免不朽时间偏倚。使用时变协变量模型作为敏感性分析。华法林平均治疗时间为1年;平均国际标准化比值在IPAH患者中为1.9,在SSc-PAH患者中为2.0。三分之二开始使用华法林的患者在最后一次研究评估前停止了治疗。与匹配的对照组相比,IPAH患者(调整后风险比,1.37;P = 0.21)或SSc-PAH患者(调整后风险比,1.60;P = 0.15)使用华法林后生存率无差异。然而,与未使用过华法林的患者相比,前一年接受华法林治疗的SSc-PAH患者(风险比,1.57;P = 0.031)或基线后任何时间接受华法林治疗的患者(风险比,1.49;P = 0.046)死亡率增加。
开始使用华法林的IPAH患者未观察到显著的生存优势。在SSc-PAH患者中,即使调整混杂因素后,长期使用华法林与未接受华法林治疗的患者相比生存率更低。