Vogel Jennifer, Ojerholm Eric, Hollander Andrew, Briola Cynthia, Mooij Rob, Bieda Michael, Kolker James, Nagda Suneel, Geiger Geoffrey, Dorsey Jay, Lustig Robert, O'Rourke Donald M, Brem Steven, Lee John, Alonso-Basanta Michelle
Department of Radiation Oncology, University of Pennsylvania, TRC-2 West, 3400 Civic Center Boulevard, Philadelphia, PA, 19104, USA.
Department of Radiation Oncology, Pennsylvania Hospital, Widener Ground Level, 800 Spruce Street, Philadelphia, PA, 19107, USA.
Radiat Oncol. 2015 Oct 31;10:221. doi: 10.1186/s13014-015-0523-4.
Stereotactic radiosurgery (SRS) is an alternative to post-operative whole brain radiation therapy (WBRT) following resection of brain metastases. At our institution, CyberKnife (CK) is considered for local treatment of large cavities ≥2 cm. In this study, we aimed to evaluate patterns of failure and characterize patients best suited to treatment with this approach.
We retrospectively reviewed 30 patients treated with CK to 33 resection cavities ≥2 cm between 2011 and 2014. Patterns of intracranial failure were analyzed in 26 patients with post-treatment imaging. Survival was estimated by the Kaplan-Meier method and prognostic factors examined with log-rank test and Cox proportional hazards model.
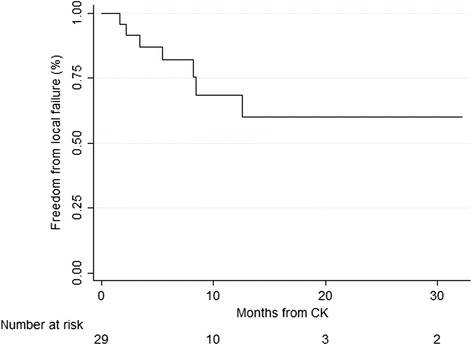
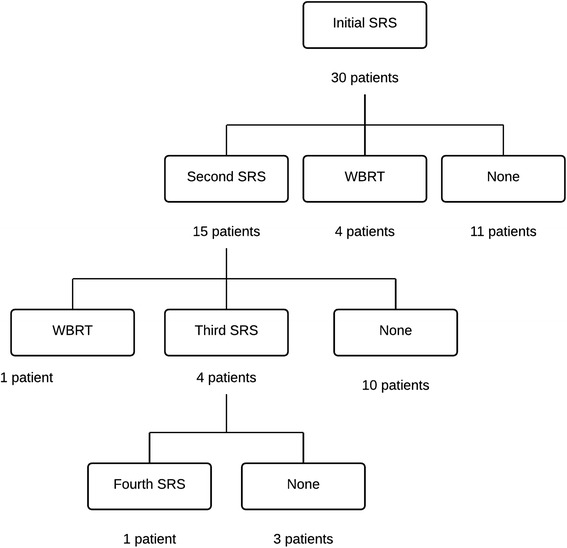
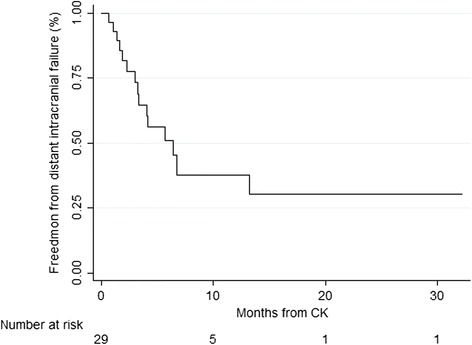
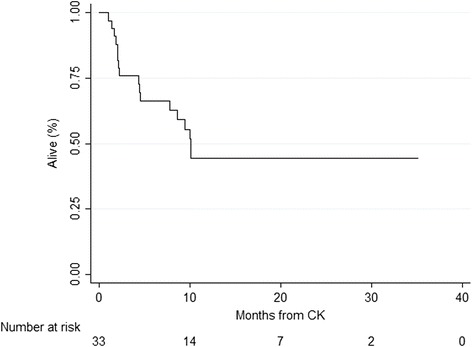
The most frequent histologies were lung (43 %) and breast (20 %). Median treatment volume was 25.1 cm(3) (range 4.7-90.9 cm(3)) and median maximal postoperative cavity diameter was 3.8 cm (range 2.8-6.7). The most common treatment was 30 Gy in 5 fractions prescribed to the 75 % isodose line. Median follow up for the entire cohort was 9.5 months (range 1.0-34.3). Local failure developed in 7 treated cavities (24 %). Neither cavity volume nor CK treatment volume was associated with local failure. Distant brain failure occurred in 20 cases (62 %) at a median of 4.2 months. There were increased rates of distant failure in patients who initially presented with synchronous metastases (p = 0.02). Leptomeningeal carcinomatosis (LMC) developed in 9 cases, (34 %). Salvage WBRT was performed in 5 cases (17 %) at a median of 5.2 months from CK. Median overall survival was 10.1 months from treatment.
This study suggests that adjuvant CK is a reasonable strategy to achieve local control in large resection cavities. Patients with synchronous metastases at the time of CK may be at higher risk for distant brain failure. The majority of cases were spared or delayed WBRT with the use of local CK therapy.
立体定向放射外科(SRS)是脑转移瘤切除术后全脑放疗(WBRT)的替代方案。在我们机构,对于直径≥2 cm的大腔隙采用射波刀(CK)进行局部治疗。在本研究中,我们旨在评估失败模式并确定最适合采用这种方法治疗的患者特征。
我们回顾性分析了2011年至2014年间接受CK治疗的30例患者的33个直径≥2 cm的切除腔隙。对26例接受治疗后影像学检查的患者分析颅内失败模式。采用Kaplan-Meier法估计生存率,并通过对数秩检验和Cox比例风险模型检查预后因素。
最常见的组织学类型为肺癌(43%)和乳腺癌(20%)。中位治疗体积为25.1 cm³(范围4.7 - 90.9 cm³),术后最大腔隙直径中位值为3.8 cm(范围2.8 - 6.7)。最常用的治疗方案是在75%等剂量线上给予5次分割、总剂量30 Gy。整个队列的中位随访时间为9.5个月(范围1.0 - 34.3)。7个接受治疗的腔隙(24%)出现局部失败。腔隙体积和CK治疗体积均与局部失败无关。20例(62%)发生远处脑转移,中位时间为4.2个月。初始表现为同时性转移瘤的患者远处失败率更高(p = 0.02)。9例(34%)发生软脑膜癌病(LMC)。5例(17%)在CK治疗后中位5.2个月时进行了挽救性WBRT。从治疗开始计算,中位总生存期为10.1个月。
本研究表明,辅助性CK是实现大切除腔隙局部控制的合理策略。接受CK治疗时存在同时性转移瘤的患者发生远处脑转移的风险可能更高。大多数病例通过局部CK治疗避免或推迟了WBRT。