Diehl Christian D, Giordano Frank A, Grosu Anca-L, Ille Sebastian, Kahl Klaus-Henning, Onken Julia, Rieken Stefan, Sarria Gustavo R, Shiban Ehab, Wagner Arthur, Beck Jürgen, Brehmer Stefanie, Ganslandt Oliver, Hamed Motaz, Meyer Bernhard, Münter Marc, Raabe Andreas, Rohde Veit, Schaller Karl, Schilling Daniela, Schneider Matthias, Sperk Elena, Thomé Claudius, Vajkoczy Peter, Vatter Hartmut, Combs Stephanie E
Department of Radiation Oncology, Technical University of Munich (TUM), Klinikum rechts der Isar, 81675 München, Germany.
Institute of Radiation Medicine (IRM), Helmholtz Zentrum München, 85764 Neuherberg, Germany.
Cancers (Basel). 2023 Jul 19;15(14):3670. doi: 10.3390/cancers15143670.
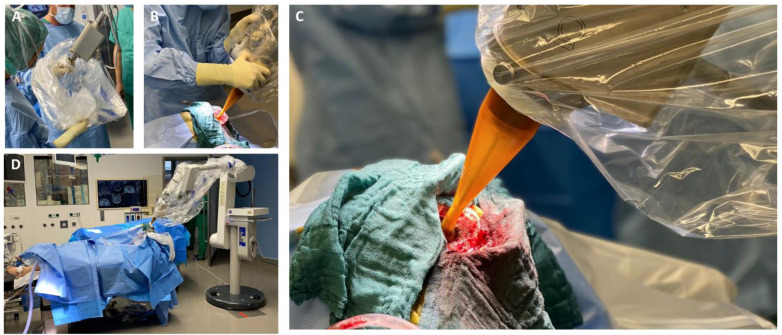
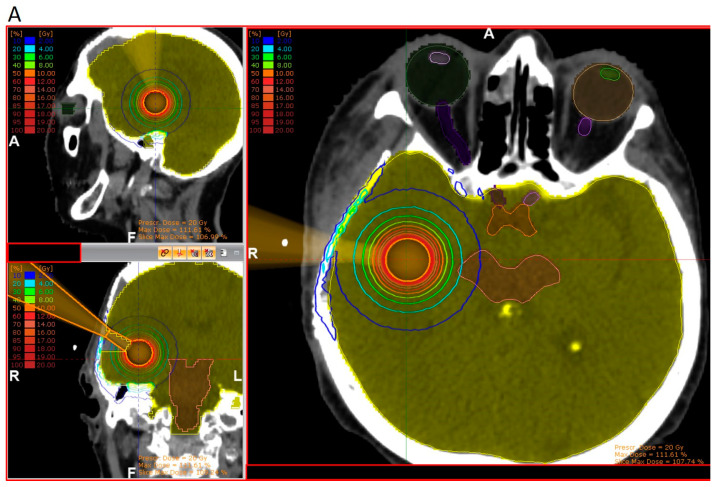
Postsurgical radiotherapy (RT) has been early proven to prevent local tumor recurrence, initially performed with whole brain RT (WBRT). Subsequent to disadvantageous cognitive sequalae for the patient and the broad distribution of modern linear accelerators, focal irradiation of the tumor has omitted WBRT in most cases. In many studies, the effectiveness of local RT of the resection cavity, either as single-fraction stereotactic radiosurgery (SRS) or hypo-fractionated stereotactic RT (hFSRT), has been demonstrated to be effective and safe. However, whereas prospective high-level incidence is still lacking on which dose and fractionation scheme is the best choice for the patient, further ablative techniques have come into play. Neoadjuvant SRS (N-SRS) prior to resection combines straightforward target delineation with an accelerated post-surgical phase, allowing an earlier start of systemic treatment or rehabilitation as indicated. In addition, low-energy intraoperative RT (IORT) on the surgical bed has been introduced as another alternative to external beam RT, offering sterilization of the cavity surface with steep dose gradients towards the healthy brain. This consensus paper summarizes current local treatment strategies for resectable brain metastases regarding available data and patient-centered decision-making.
术后放疗(RT)早已被证实可预防局部肿瘤复发,最初采用的是全脑放疗(WBRT)。鉴于其对患者存在不利的认知后遗症,以及现代直线加速器的广泛应用,多数情况下肿瘤的局部照射已不再采用WBRT。在许多研究中,已证明切除腔的局部放疗,无论是单次分割立体定向放射外科手术(SRS)还是低分割立体定向放疗(hFSRT),都是有效且安全的。然而,由于仍缺乏关于哪种剂量和分割方案对患者是最佳选择的前瞻性高水平研究,进一步的消融技术开始发挥作用。切除术前的新辅助SRS(N-SRS)将直接的靶区勾画与加速的术后阶段相结合,从而能根据需要更早地开始全身治疗或康复。此外,手术床上的低能术中放疗(IORT)已作为外照射放疗的另一种替代方法被引入,它能使腔表面消毒,且对健康脑组织的剂量梯度陡峭。本共识文件根据现有数据和以患者为中心的决策制定,总结了可切除脑转移瘤目前的局部治疗策略。