Allan Philip D, Faulkner James, O'Donnell Terrence, Lanford Jeremy, Wong Lai-Kin, Saleem Saqib, Woolley Brandon, Lambrick Danielle, Stoner Lee, Tzeng Yu-Chieh
Centre for Translational Physiology, University of Otago, Wellington, New Zealand Department of Surgery and Anaesthesia, University of Otago, Wellington, New Zealand.
Department of Sport and Exercise, University of Winchester, Winchester, UK.
Physiol Rep. 2015 Nov;3(11). doi: 10.14814/phy2.12602.
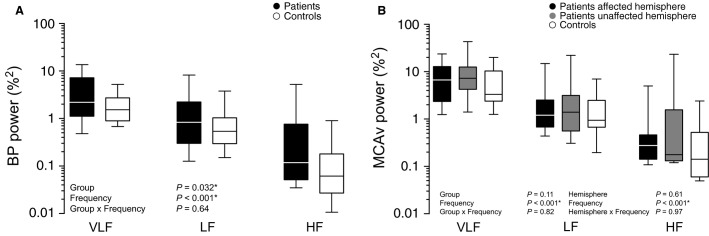
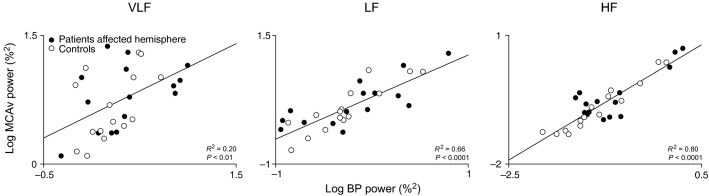
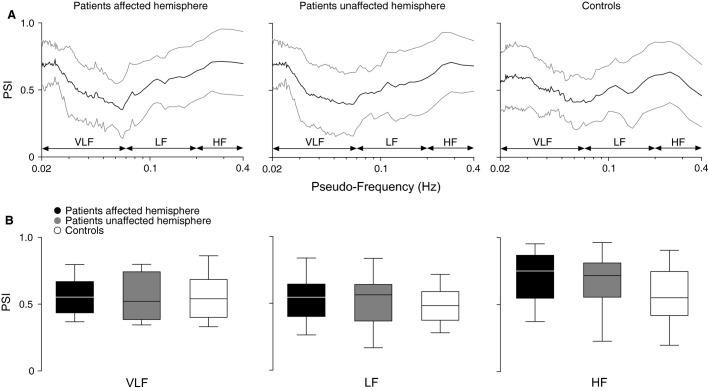
We investigated if hemodynamic variability, cerebral blood flow (CBF) regulation, and their interrelationships differ between patients with transient ischemic attack (TIA) and controls. We recorded blood pressure (BP) and bilateral middle cerebral artery flow velocity (MCAv) in a cohort of TIA patients (n = 17), and age-matched controls (n = 15). Spontaneous fluctuations in BP and MCAv were characterized by spectral power analysis, and CBF regulation was assessed by wavelet phase synchronization analysis in the very low- (0.02-0.07 Hz), low- (0.07-0.20 Hz), and high-frequency (0.20-0.40 Hz) ranges. Furthermore, cerebrovascular CO2 reactivity was assessed as a second metric of CBF regulation by inducing hypercapnia with 8% CO2 inhalation followed by hyperventilation driven hypocapnia. We found that TIA was associated with higher BP power (group effect, P < 0.05), but not MCAv power (P = 0.11). CBF regulation (assessed by wavelet phase synchronization and CO2 reactivity) was intact in patients (all P ≥ 0.075) across both hemispheres (all P ≥ 0.51). Pooled data (controls and affected hemisphere of patients) showed that BP and MCAv power were positively correlated at all frequency ranges (R(2) = 0.20-0.80, all P < 0.01). Furthermore, LF phase synchronization index was a significant determinant of MCAv power (P < 0.05), while VLF and HF phase synchronization index, and TIA were not (all P ≥ 0.50). These results indicate that CBF stability and control is maintained in TIA patients, but BPV is markedly elevated. BPV attenuation may be an important therapeutic strategy for enhancing secondary stroke prevention in patients who suffer a TIA.
我们研究了短暂性脑缺血发作(TIA)患者与对照组之间的血流动力学变异性、脑血流量(CBF)调节及其相互关系是否存在差异。我们记录了一组TIA患者(n = 17)和年龄匹配的对照组(n = 15)的血压(BP)和双侧大脑中动脉血流速度(MCAv)。通过频谱功率分析表征BP和MCAv的自发波动,并通过小波相位同步分析在极低频(0.02 - 0.07Hz)、低频(0.07 - 0.20Hz)和高频(0.20 - 0.40Hz)范围内评估CBF调节。此外,通过吸入8% CO₂诱导高碳酸血症,随后进行过度通气驱动的低碳酸血症,将脑血管CO₂反应性评估为CBF调节的第二个指标。我们发现TIA与较高的BP功率相关(组效应,P < 0.05),但与MCAv功率无关(P = 0.11)。患者两侧半球的CBF调节(通过小波相位同步和CO₂反应性评估)均完好(所有P≥0.075)(所有P≥0.51)。汇总数据(对照组和患者患侧半球)显示,BP和MCAv功率在所有频率范围内均呈正相关(R² = 0.20 - 0.80,所有P < 0.01)。此外,低频相位同步指数是MCAv功率的重要决定因素(P < 0.05),而极低频和高频相位同步指数以及TIA则不是(所有P≥0.50)。这些结果表明,TIA患者的CBF稳定性和调节功能得以维持,但BPV明显升高。BPV衰减可能是增强TIA患者二级卒中预防的重要治疗策略。