Sanders Eduard J, Wahome Elizabeth, Powers Kimberly A, Werner Lisa, Fegan Greg, Lavreys Ludo, Mapanje Clement, McClelland R Scott, Garrett Nigel, Miller William C, Graham Susan M
aCentre for Geographic Medicine Research - Coast, Kenya Medical Research Institute (KEMRI) - Kilifi, Kenya bNuffield Department of Medicine, University of Oxford, Headington, UK cDepartment of Global Health, Academic Medical Centre, University of Amsterdam, Amsterdam, the Netherlands dDepartment of Epidemiology, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA eCentre for the AIDS Programme of Research in South Africa (CAPRISA), University of KwaZulu-Natal, Durban, South Africa fMaisha Consulting bvba, Tildonk, Belgium gUNC Project Malawi, Lilongwe, Malawi hDepartments of Medicine, Global Health, and Epidemiology, University of Washington, Seattle, Washington iDepartment of Medicine, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA.
AIDS. 2015 Dec;29 Suppl 3(0 3):S221-30. doi: 10.1097/QAD.0000000000000924.
Patients with acute HIV-1 infection (AHI) have elevated infectivity, but cannot be diagnosed using antibody-based testing. Approaches to screen patients for AHI are urgently needed to enable counselling and treatment to reduce onward transmission.
We pooled data from four African studies of high-risk adults that evaluated symptoms and signs compatible with acute retroviral syndrome and tested for HIV-1 at each visit. AHI was defined as detectable plasma viral load or p24 antigen in an HIV-1-antibody-negative patient who subsequently seroconverted. Using generalized estimating equation, we identified symptoms, signs, and demographic factors predictive of AHI, adjusting for study site. We assigned a predictor score to each statistically significant predictor based on its beta coefficient, summing predictor scores to calculate a risk score for each participant. We evaluated the performance of this algorithm overall and at each site.
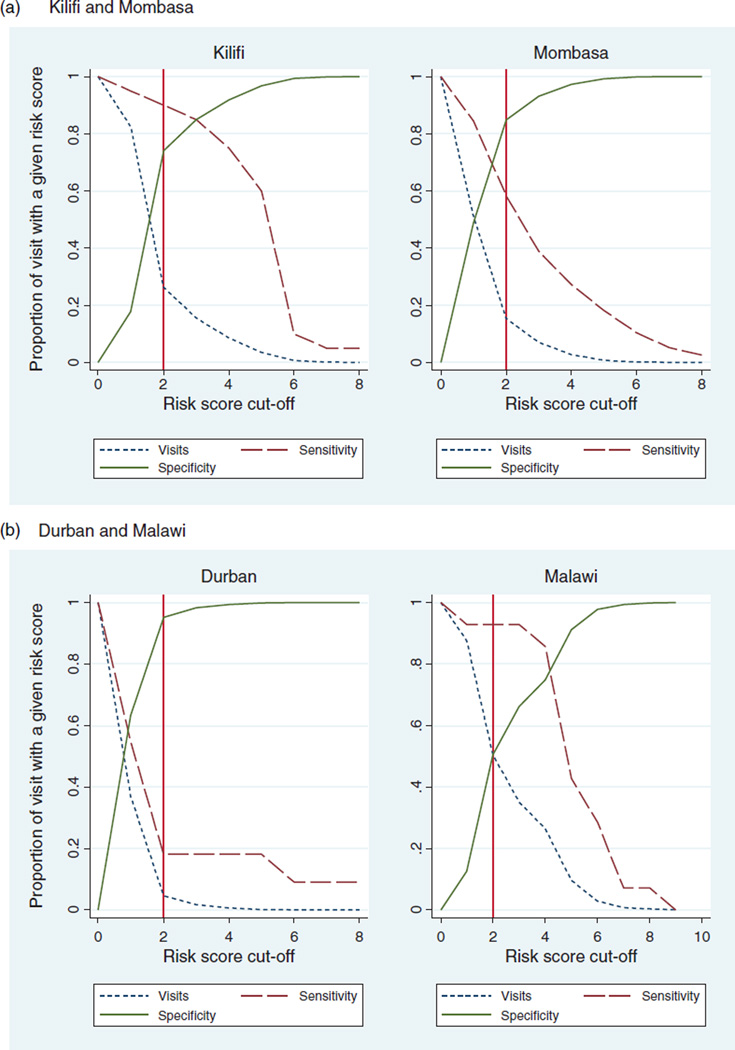
We compared 122 AHI visits with 45 961 visits by uninfected patients. Younger age (18-29 years), fever, fatigue, body pains, diarrhoea, sore throat, and genital ulcer disease were independent predictors of AHI. The overall area under the receiver operating characteristics curve (AUC) for the algorithm was 0.78, with site-specific AUCs ranging from 0.61 to 0.89. A risk score of at least 2 would indicate AHI testing for 5-50% of participants, substantially decreasing the number needing testing.
Our targeted risk score algorithm based on seven characteristics reduced the number of patients needing AHI testing and had good performance overall. We recommend this risk score algorithm for use by HIV programs in sub-Saharan Africa with capacity to test high-risk patients for AHI.
急性HIV-1感染(AHI)患者具有较高的传染性,但无法通过基于抗体的检测进行诊断。迫切需要采用相关方法来筛查AHI患者,以便为其提供咨询和治疗,从而减少病毒的进一步传播。
我们汇总了四项针对非洲高危成年人的研究数据,这些研究评估了与急性逆转录病毒综合征相符的症状和体征,并在每次就诊时进行HIV-1检测。AHI被定义为在随后发生血清转化的HIV-1抗体阴性患者中检测到血浆病毒载量或p24抗原。我们使用广义估计方程,确定了预测AHI的症状、体征和人口统计学因素,并对研究地点进行了校正。我们根据每个具有统计学意义的预测因素的β系数为其分配一个预测分数,将预测分数相加,为每个参与者计算一个风险分数。我们评估了该算法在总体以及各个研究地点的性能。
我们将122次AHI就诊与未感染患者的45961次就诊进行了比较。年龄较小(18 - 29岁)、发热、疲劳、身体疼痛、腹泻、喉咙痛和生殖器溃疡病是AHI的独立预测因素。该算法的总体受试者工作特征曲线下面积(AUC)为0.78,各研究地点的AUC范围为0.61至0.89。风险分数至少为2表明5% - 50%的参与者需要进行AHI检测,这将大幅减少需要检测的人数。
我们基于七个特征的目标风险评分算法减少了需要进行AHI检测的患者数量,总体性能良好。我们建议撒哈拉以南非洲地区有能力为高危患者进行AHI检测的HIV项目使用这种风险评分算法。