Marik Paul E, Cavallazzi Rodrigo
Division of Pulmonary and Critical Care Medicine, Eastern Virginia Medical School, Norfolk, Virginia, United States of America.
Division of Pulmonary, Critical Care and Sleep Medicine, University of Louisville, Louisville, Kentucky, United States of America.
PLoS One. 2015 Nov 20;10(11):e0143252. doi: 10.1371/journal.pone.0143252. eCollection 2015.
Patients who have had an unprovoked deep venous thrombosis (DVT) or pulmonary embolus (PE) are at a high risk for recurrent venous thromboembolism (VTE). Extended "life-long" anticoagulation has been recommended in these patients. However, the risk benefit ratio of this approach is controversial and the role of the direct oral anticoagulants (DOACs) and aspirin is unclear. Furthermore, in some patients with a "weak provoking factor" there is clinical equipoise regarding continuation or cessation of anticoagulant therapy after treatment of the acute VTE event.
A systematic review and meta-analysis to determine the risks (major bleeding) and benefits (recurrent VTE and mortality) of extended anticoagulation with vitamin k antagonists (VKA), DOACs and aspirin in patients with an unprovoked VTE and in those patients with clinical equipoise regarding continuation or cessation of anticoagulant therapy. In addition, we sought to determine the risk of recurrent VTE events once extended anti-thrombotic therapy was discontinued.
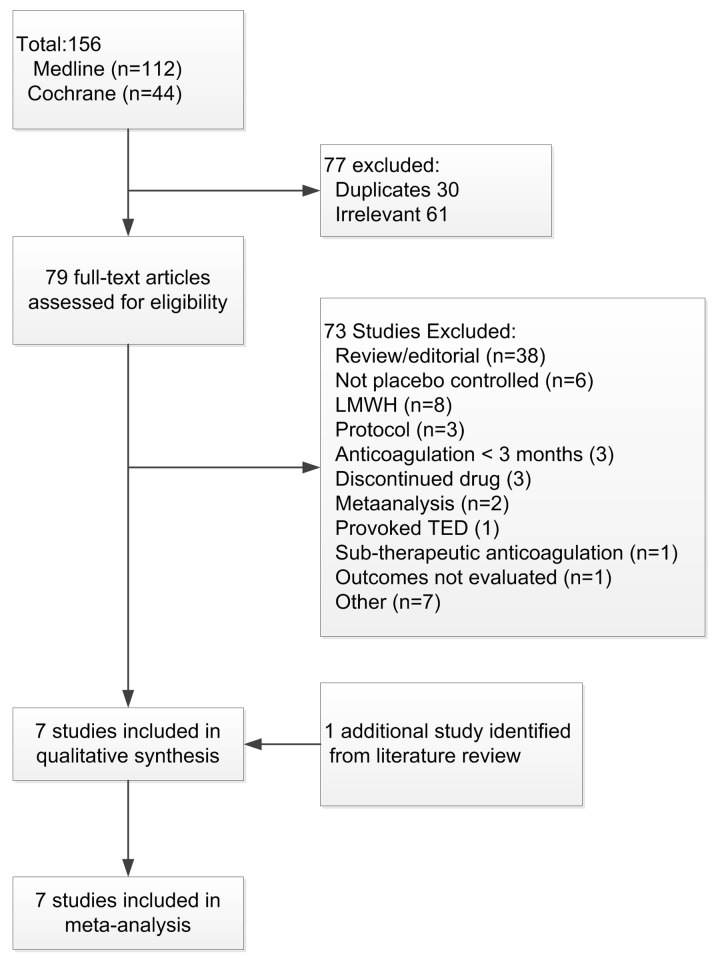
MEDLINE, Cochrane Register of Controlled Trials, citation review of relevant primary and review articles.
Randomized placebo-controlled trials (RCTs) that compared the risk of recurrent VTE in patients with an unprovoked DVT or PE who had been treated for at least 3 months with a VKA or a DOAC and were then randomized to receive an oral anti-thrombotic agent or placebo for at least 6 additional months. We included studies that included patients in whom clinical equipoise existed regarding the continuation or cessation of anticoagulant therapy.
Independent extraction of articles by both authors using predefined data fields, including study quality indicators. Data were abstracted on study size, study setting, initial event (DVT or PE), percentage of patients where the initial VTE event was unprovoked, the number of recurrent VTE events, major bleeds and mortality during the period of extended anticoagulation in the active treatment and placebo arms. In addition, we recorded the event rate once extended treatment was stopped. Meta-analytic techniques were used to summarize the data. Studies were grouped according to the type of anti-thrombotic agent.
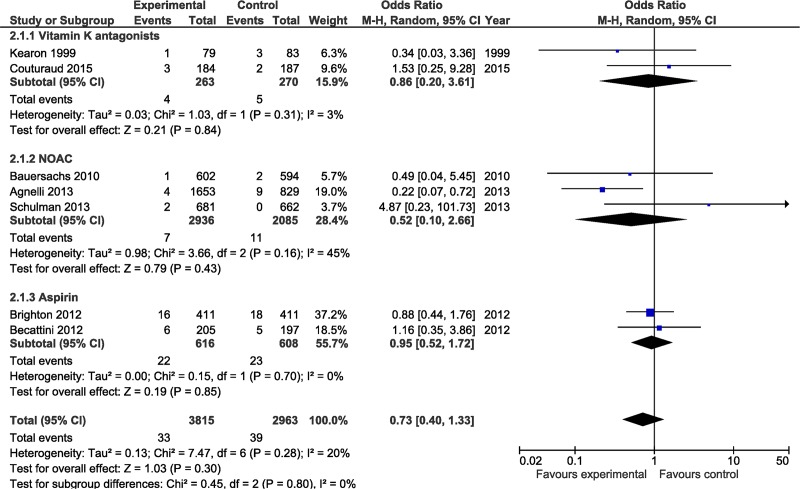
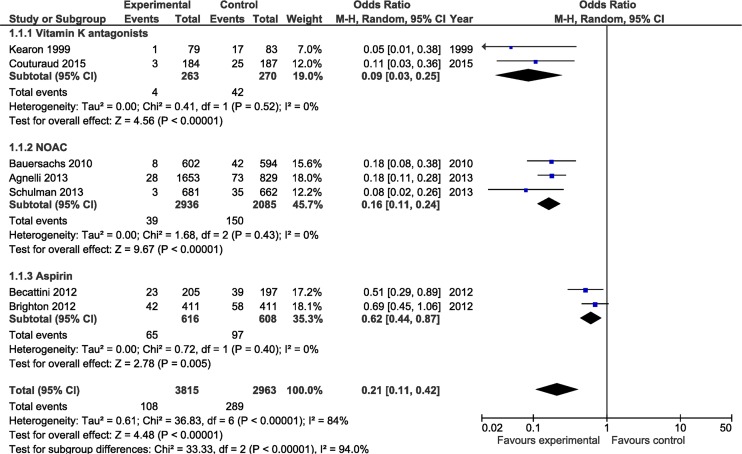
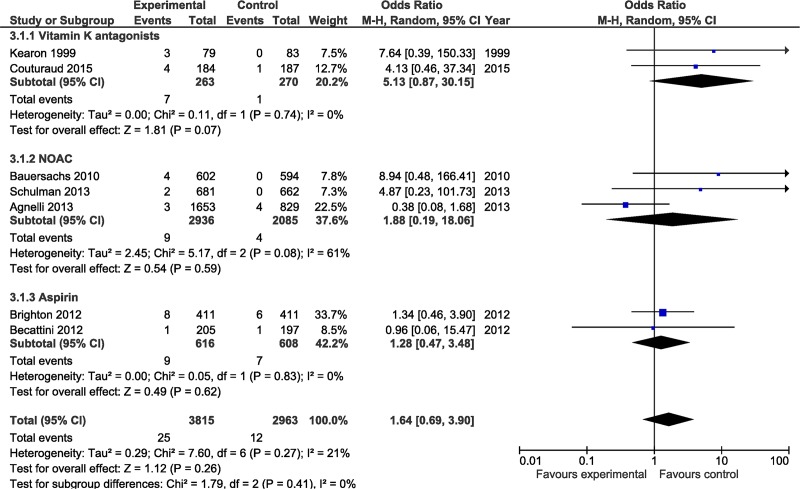
Seven studies which enrolled 6778 patients met our inclusion criteria; two studies evaluated the extended use of Coumadin, three studies evaluated a DOAC and two studies evaluated the use of aspirin. The duration of followup varied from 6 to 37 months. In the Coumadin and aspirin studies 100% of the randomized patients had an unprovoked VTE, while in the DOAC studies between 73.5% and 93.2% of the VTE events were unprovoked. In the control group recurrent VTE occurred in 9.7% of patients compared to 2.8% in the active treatment group (OR 0.21; 95% CI 0.11-0.42, p<0.0001). VKA, DOACs and aspirin significantly reduced the risk of recurrent VTE, with VKA and DOACs being significantly more effective than aspirin. Major bleeding events occurred in 12 patients in the control group (0.4%) and 25 of 3815 (0.6%) patients in the active treatment group (OR 1.64; 95% CI 0.69-3.90, NS). There were 39 (1.3%) deaths in control patients and 33 (0.9%) deaths in the anti-thrombotic group during the treatment period (OR 0.73; 95% CI 0.40-1.33, NS). Patients whose initial VTE event was a PE were more likely to have a recurrent PE than a DVT. The annualized event rate after discontinuation of extended antithrombotic therapy was 4.4% in the control group and 6.5% in the active treatment arm.
VKA, DOACs and aspirin significantly reduced the risk of recurrent VTE, with DOACs and VKA being more effective than aspirin. The decision regarding life-long anticoagulation following an unprovoked DVT or PE should depend on the patients' risk for recurrent PE as well as the patients' values and preferences.
发生不明原因的深静脉血栓形成(DVT)或肺栓塞(PE)的患者,复发静脉血栓栓塞症(VTE)的风险很高。已建议对这些患者进行长期“终身”抗凝治疗。然而,这种方法的风险效益比存在争议,直接口服抗凝剂(DOACs)和阿司匹林的作用尚不清楚。此外,在一些有“轻度诱发因素”的患者中,对于急性VTE事件治疗后抗凝治疗的继续或停止存在临床平衡。
进行一项系统评价和荟萃分析,以确定在不明原因VTE患者以及在抗凝治疗的继续或停止存在临床平衡的患者中,使用维生素K拮抗剂(VKA)、DOACs和阿司匹林进行长期抗凝的风险(大出血)和益处(复发性VTE和死亡率)。此外,我们试图确定延长抗血栓治疗停药后复发性VTE事件的风险。
MEDLINE、Cochrane对照试验注册库、对相关原始文献和综述文章的引文回顾。
随机安慰剂对照试验(RCTs),比较不明原因DVT或PE患者接受VKA或DOAC治疗至少3个月后,再随机接受口服抗血栓药物或安慰剂至少6个月的复发性VTE风险。我们纳入了在抗凝治疗的继续或停止方面存在临床平衡的患者的研究。
两位作者使用预定义的数据字段独立提取文章,包括研究质量指标。提取的数据包括研究规模、研究背景、初始事件(DVT或PE)、初始VTE事件为不明原因的患者百分比、复发性VTE事件数量、在积极治疗组和安慰剂组长期抗凝期间的大出血和死亡率。此外,我们记录了延长治疗停止后的事件发生率。使用荟萃分析技术汇总数据。根据抗血栓药物的类型对研究进行分组。
七项纳入6778例患者的研究符合我们的纳入标准;两项研究评估了华法林的长期使用,三项研究评估了一种DOAC,两项研究评估了阿司匹林的使用。随访时间从6个月到37个月不等。在华法林和阿司匹林研究中,100%的随机分组患者发生不明原因的VTE,而在DOAC研究中,73.5%至93.2%的VTE事件为不明原因。对照组中9.7%的患者发生复发性VTE,而积极治疗组为2.8%(OR 0.21;95%CI 0.11 - 0.42,p<0.0001)。VKA、DOACs和阿司匹林显著降低了复发性VTE的风险,VKA和DOACs比阿司匹林更有效。对照组有12例患者(0.4%)发生大出血事件,积极治疗组3815例患者中有25例(0.6%)发生(OR 1.64;95%CI 0.69 - 3.90,无统计学意义)。治疗期间对照组有39例(1.3%)死亡,抗血栓组有33例(0.9%)死亡(OR 0.73;95%CI 0.40 - 1.33,无统计学意义)。初始VTE事件为PE的患者比DVT患者更有可能复发PE。延长抗血栓治疗停药后的年化事件发生率在对照组为4.4%,在积极治疗组为6.5%。
VKA、DOACs和阿司匹林显著降低了复发性VTE的风险,DOACs和VKA比阿司匹林更有效。不明原因DVT或PE后终身抗凝的决策应取决于患者复发PE的风险以及患者的价值观和偏好。