Schur Nadine, Mylne Adrian, Mushati Phyllis, Takaruza Albert, Ward Helen, Nyamukapa Constance, Gregson Simon
Department of Infectious Disease Epidemiology, Imperial College London, London, UK.
Biomedical Research and Training Institute, Harare, Zimbabwe.
J Int AIDS Soc. 2015 Nov 20;18(1):20063. doi: 10.7448/IAS.18.1.20063. eCollection 2015.
Intensified poverty arising from economic decline and crisis may have contributed to reductions in HIV prevalence in Zimbabwe.
To assess the impact of the economic decline on household wealth and prevalent HIV infection using data from a population-based open cohort.
Household wealth was estimated using data from a prospective household census in Manicaland Province (1998 to 2011). Temporal trends in summed asset ownership indices for sellable, non-sellable and all assets combined were compared for households in four socio-economic strata (small towns, agricultural estates, roadside settlements and subsistence farming areas). Multivariate logistic random-effects models were used to measure differences in individual-level associations between prevalent HIV infection and place of residence, absolute wealth group and occupation.
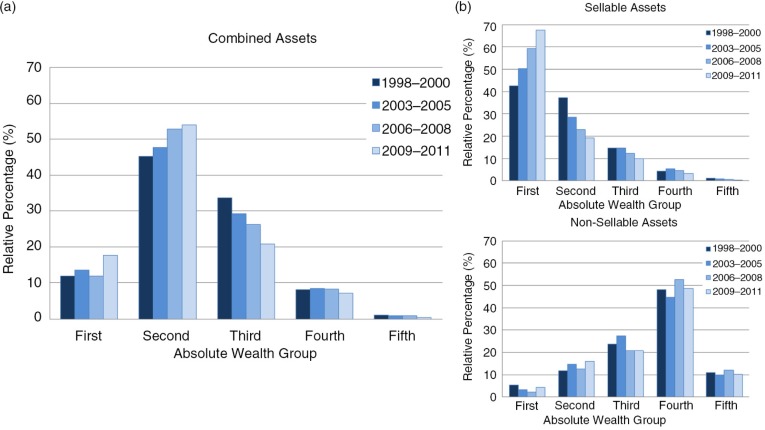
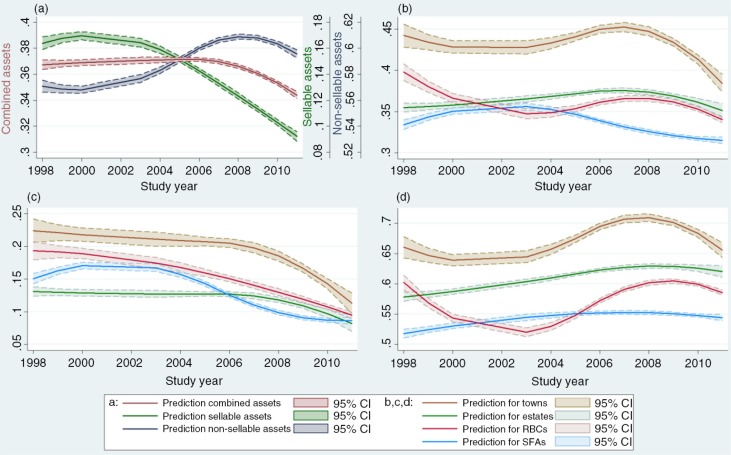
Household mean asset scores remained similar at around 0.37 (on a scale of 0 to 1) up to 2007 but decreased to below 0.35 thereafter. Sellable assets fell substantially from 2004 while non-sellable assets continued increasing until 2008. Small-town households had the highest wealth scores but the gap to other locations decreased over time, especially for sellable assets. Concurrently, adult HIV prevalence fell from 22.3 to 14.3%. HIV prevalence was highest in better-off locations (small towns) but differed little by household wealth or occupation. Initially, HIV prevalence was elevated in women from poorer households and lower in men in professional occupations. However, most recently (2009 to 2011), men and women in the poorest households had lower HIV prevalence and men in professional occupations had similar prevalence to unemployed men.
The economic crisis drove more households into extreme poverty. However, HIV prevalence fell in all socio-economic locations and sub-groups, and there was limited evidence that increased poverty contributed to HIV prevalence decline.
经济衰退和危机导致的贫困加剧可能促使津巴布韦的艾滋病毒感染率下降。
利用基于人群的开放队列数据,评估经济衰退对家庭财富和艾滋病毒感染流行情况的影响。
使用马尼卡兰省(1998年至2011年)前瞻性家庭普查数据估算家庭财富。比较了四个社会经济阶层(小镇、农业庄园、路边定居点和自给农业区)家庭可出售资产、不可出售资产以及所有资产总和的所有权指数的时间趋势。采用多变量逻辑随机效应模型来衡量艾滋病毒感染流行情况与居住地点、绝对财富组和职业之间个体层面关联的差异。
到2007年,家庭平均资产得分在0至1的范围内保持在约0.37左右,但此后降至0.35以下。可出售资产自2004年起大幅下降,而不可出售资产在2008年之前持续增加。小镇家庭的财富得分最高,但与其他地区的差距随着时间的推移而缩小,尤其是可出售资产方面。与此同时,成人艾滋病毒感染率从22.3%降至14.3%。艾滋病毒感染率在较富裕地区(小镇)最高,但在家庭财富或职业方面差异不大。最初,贫困家庭的女性艾滋病毒感染率较高,从事专业职业的男性感染率较低。然而,最近(2009年至2011年),最贫困家庭的男性和女性艾滋病毒感染率较低,从事专业职业的男性与失业男性的感染率相似。
经济危机使更多家庭陷入极端贫困。然而,所有社会经济地区和亚组的艾滋病毒感染率均有所下降,而且几乎没有证据表明贫困加剧导致了艾滋病毒感染率下降。