Department of Clinical Immunology & Rheumatology , Academic Medical Center, University of Amsterdam , Amsterdam , The Netherlands ; Department of Rheumatology , Hospital Garcia de Orta , Almada , Portugal.
Department of Clinical Immunology & Rheumatology , Academic Medical Center, University of Amsterdam , Amsterdam , The Netherlands ; Department of Rheumatology , Atrium Medical Center , Heerlen , The Netherlands.
RMD Open. 2015 Nov 18;1(1):e000155. doi: 10.1136/rmdopen-2015-000155. eCollection 2015.
To compare discontinuation rates of first and second biologics in rheumatoid arthritis (RA) by tumour-necrosis factor inhibitor (TNFi) status and identify predictors and reasons for discontinuation.
From 1998 to 2011, self-reported medication use for RA was assessed every 6 months via questionnaire in a longitudinal study in the USA. Time-on-drug analyses were conducted for individual biologics and groups, and annual rates reported. Time to discontinuation of TNFi and non-TNFi was compared, unadjusted and adjusted using propensity score analyses. Baseline and time-varying predictors of biologic discontinuation were derived through Cox regression.
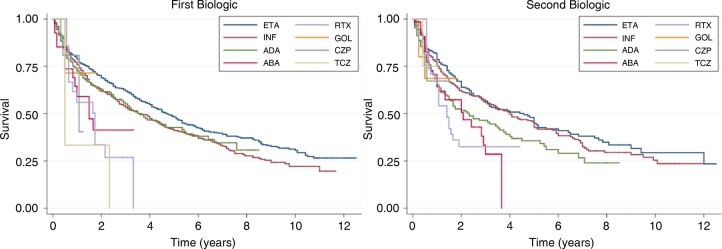
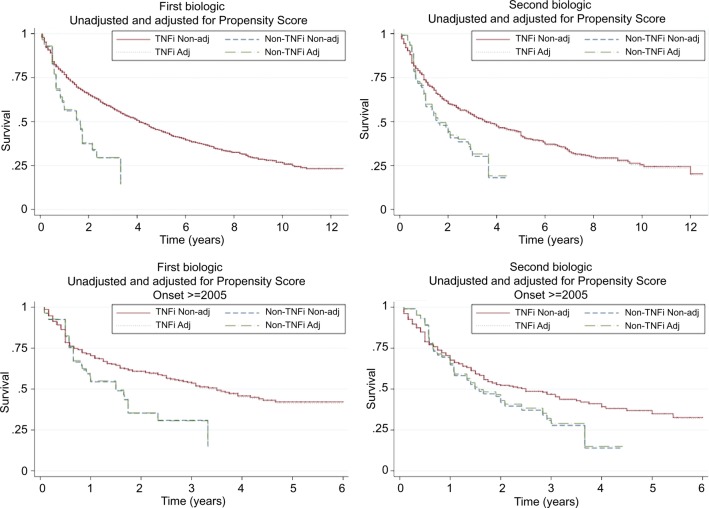
Of 2281 patients initiating their first biologic, 1100 (48%) discontinued and of 1097 initiating a second biologic, 537 (49%) discontinued. The annual discontinuation rate was 17% (median 4 years) for first biologic and 20% (median 3.3 years) for second biologic. TNFi had lower discontinuation rates than non-TNFi after propensity score adjustment: HR for first biologic 0.49 (0.34 to 0.71) and 0.68 (0.51 to 0.90) for second biologic. The annual discontinuation rate was significantly lower in patients starting their first biologic before January 2005 vs after (16 vs 25%, p=0.005). Predictors of discontinuation for the first biologic included smoking, higher comorbidity index, worse overall health and not using concomitant methotrexate.
In this large cohort, patients with RA tended to remain on their first and second biologics for relatively long periods suggesting the drugs' effectiveness. Discontinuation rates were lower in patients using TNFi, and all rates increased after January 2005 when the number of biologics available increased.
比较肿瘤坏死因子抑制剂(TNFi)状态下类风湿关节炎(RA)患者首次和二次使用生物制剂的停药率,并确定停药的预测因素和原因。
1998 年至 2011 年,在美国一项纵向研究中,每 6 个月通过问卷调查评估 RA 患者的自我报告用药情况。对个体生物制剂和组进行药物使用时间分析,并报告年度停药率。比较 TNFi 和非 TNFi 的停药时间,未调整和使用倾向评分分析调整后。通过 Cox 回归得出生物制剂停药的基线和时变预测因素。
在 2281 例首次使用生物制剂的患者中,有 1100 例(48%)停药,在 1097 例开始使用第二种生物制剂的患者中,有 537 例(49%)停药。首次生物制剂的年停药率为 17%(中位数 4 年),第二次生物制剂为 20%(中位数 3.3 年)。经倾向评分调整后,TNFi 的停药率低于非 TNFi:首次生物制剂的 HR 为 0.49(0.34 至 0.71)和 0.68(0.51 至 0.90),第二次生物制剂。与 2005 年 1 月前开始首次生物制剂治疗的患者相比,该年开始首次生物制剂治疗的患者的年停药率显著降低(16%比 25%,p=0.005)。首次生物制剂停药的预测因素包括吸烟、更高的合并症指数、更差的整体健康状况和不使用伴随甲氨蝶呤。
在这项大型队列研究中,RA 患者倾向于长期使用他们的第一和第二种生物制剂,这表明这些药物具有有效性。使用 TNFi 的患者停药率较低,且所有停药率均在 2005 年 1 月之后增加,当时可用的生物制剂数量增加。