Raol Nikhila, Zogg Cheryl K, Boss Emily F, Weissman Joel S
Center for Surgery and Public Health, Harvard Medical School and Harvard T. H. Chan School of Public Health, Department of Surgery, Brigham & Women's Hospital, Boston, Massachusetts, USA Massachusetts Eye and Ear Infirmary, Department of Otolaryngology, Harvard Medical School, Boston, Massachusetts, USA
Center for Surgery and Public Health, Harvard Medical School and Harvard T. H. Chan School of Public Health, Department of Surgery, Brigham & Women's Hospital, Boston, Massachusetts, USA.
Otolaryngol Head Neck Surg. 2016 Mar;154(3):486-93. doi: 10.1177/0194599815621739. Epub 2015 Dec 23.
To ascertain whether hospital type is associated with differences in total cost and outcomes for inpatient tonsillectomy.
Cross-sectional analysis of the 2006, 2009, and 2012 Kids' Inpatient Database (KID).
Children ≤18 years of age undergoing tonsillectomy with/without adenoidectomy were included. Risk-adjusted generalized linear models assessed for differences in hospital cost and length of stay (LOS) among children managed by (1) non-children's teaching hospitals (NCTHs), (2) children's teaching hospitals (CTHs), and (3) nonteaching hospitals (NTHs). Risk-adjusted logistic regression compared the odds of major perioperative complications (hemorrhage, respiratory failure, death). Models accounted for clustering of patients within hospitals, were weighted to provide national estimates, and controlled for comorbidities.
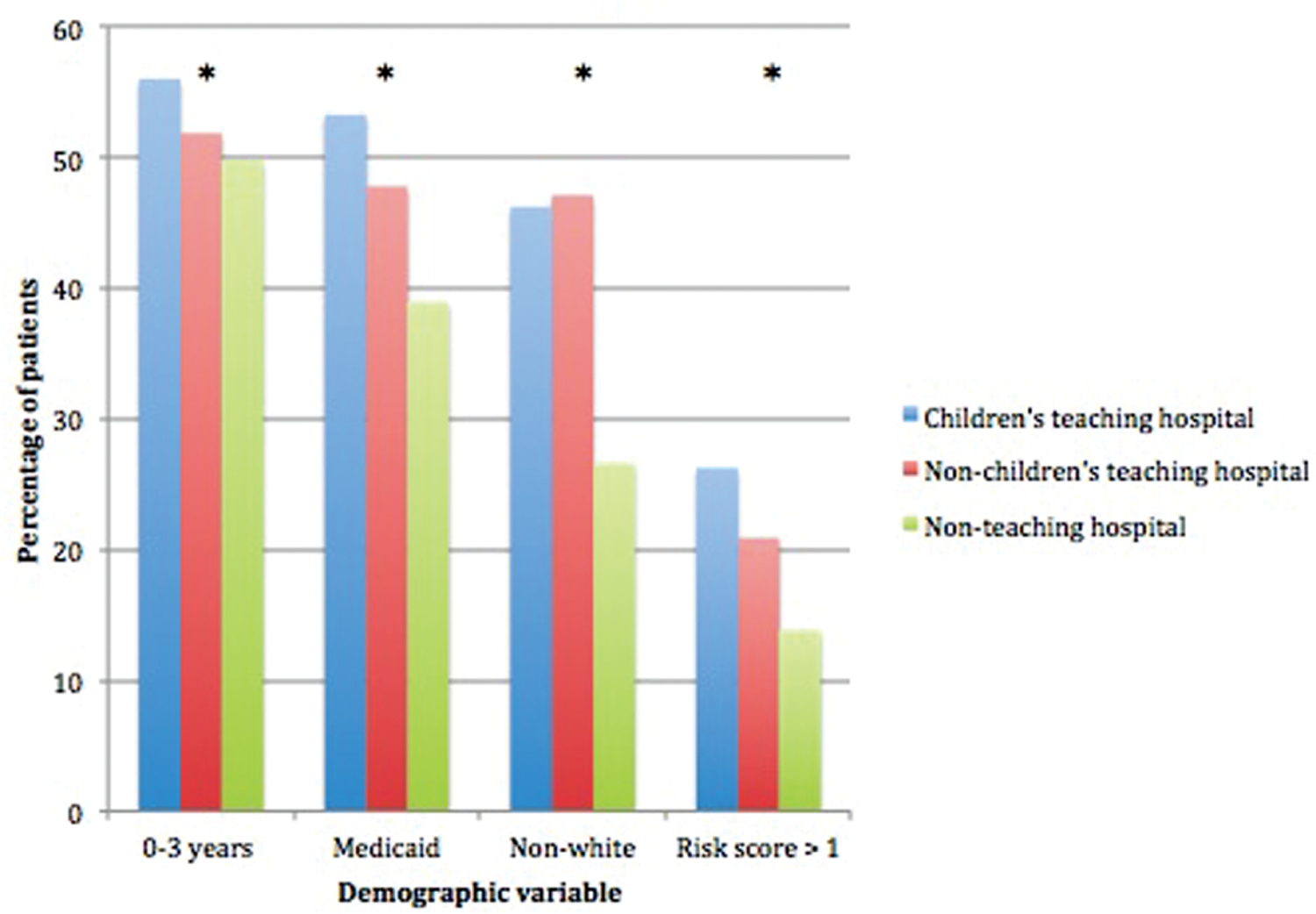
The 25,685 tonsillectomies recorded in the KID yielded a national estimate of 40,591 inpatient tonsillectomies performed in 2006, 2009, and 2012. The CTHs had significantly higher risk-adjusted total cost and LOS per tonsillectomy compared with NCTHs and NTHs ($9423.34/2.8 days, $6250.78/2.11 days, and $5905.10/2.08 days, respectively; P < .001). The CTHs had higher odds of complications compared with NCTHs (odds ratio [OR], 1.48; 95% CI, 1.15-1.91; P = .002) but not when compared with NTHs (OR, 1.19; 95% CI, 0.89-1.59; P = .23). The CTHs were significantly more likely to care for patients with comorbidities (P < .001).
Significant differences in costs, outcomes, and patient factors exist for inpatient tonsillectomy based on hospital type. Although reasons for these differences are not discernable using isolated claims data, findings provide a foundation to further evaluate patient, institutional, and system-level factors that may reduce cost of care and improve value for inpatient tonsillectomy.
确定医院类型是否与住院扁桃体切除术的总成本及治疗结果差异相关。
对2006年、2009年和2012年儿童住院数据库(KID)进行横断面分析。
纳入年龄≤18岁接受或未接受腺样体切除术的扁桃体切除术患儿。风险调整后的广义线性模型评估了由以下三类医院管理的儿童在医院成本和住院时间(LOS)方面的差异:(1)非儿童教学医院(NCTH)、(2)儿童教学医院(CTH)和(3)非教学医院(NTH)。风险调整后的逻辑回归比较了围手术期主要并发症(出血、呼吸衰竭、死亡)的发生几率。模型考虑了医院内患者的聚集情况,进行加权以提供全国估计值,并对合并症进行了控制。
KID记录的25685例扁桃体切除术得出2006年、2009年和2012年全国住院扁桃体切除术估计为40591例。与NCTH和NTH相比,CTH每例扁桃体切除术的风险调整后总成本和住院时间显著更高(分别为9423.34美元/2.8天、6250.78美元/2.11天和5905.10美元/2.08天;P < 0.001)。与NCTH相比,CTH并发症发生几率更高(优势比[OR],1.48;95%可信区间[CI],1.15 - 1.91;P = 0.002),但与NTH相比则不然(OR,1.19;95% CI,0.89 - 1.59;P =
0.23)。CTH显著更有可能护理患有合并症的患者(P < 0.001)。
基于医院类型,住院扁桃体切除术在成本、治疗结果和患者因素方面存在显著差异。尽管使用孤立的索赔数据无法明确这些差异的原因,但研究结果为进一步评估可能降低护理成本并提高住院扁桃体切除术价值的患者、机构和系统层面因素提供了基础。