Nakajima Kenichi, Nakata Tomoaki, Matsuo Shinro, Jacobson Arnold F
Department of Nuclear Medicine, Kanazawa University Hospital, 13-1 Takara-machi, Kanazawa 920-8641, Japan
Hakodate Goryoukaku Hospital, Hakodate-City, Japan.
Eur Heart J Cardiovasc Imaging. 2016 Oct;17(10):1138-45. doi: 10.1093/ehjci/jev322. Epub 2015 Dec 24.
(123)I meta-iodobenzylguanidine (MIBG) imaging has been extensively used for prognostication in patients with chronic heart failure (CHF). The purpose of this study was to create mortality risk charts for short-term (2 years) and long-term (5 years) prediction of cardiac mortality.
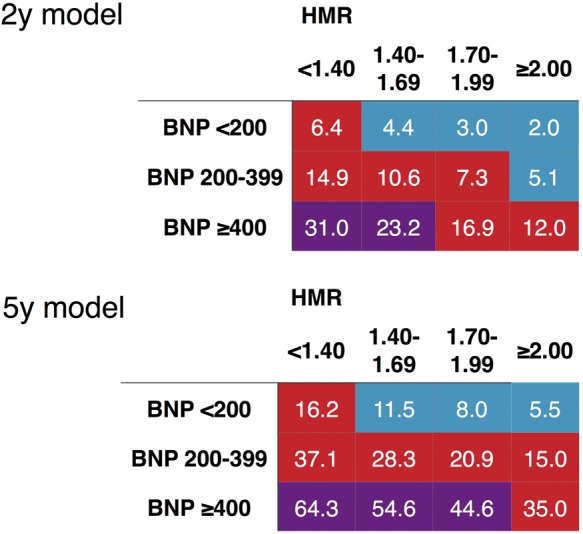
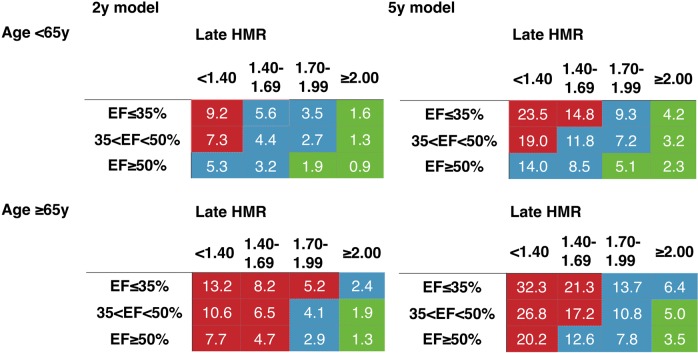
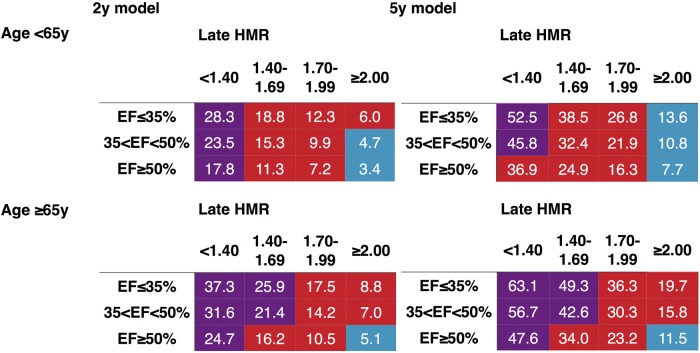
Using a pooled database of 1322 CHF patients, multivariate analysis, including (123)I-MIBG late heart-to-mediastinum ratio (HMR), left ventricular ejection fraction (LVEF), and clinical factors, was performed to determine optimal variables for the prediction of 2- and 5-year mortality risk using subsets of the patients (n = 1280 and 933, respectively). Multivariate logistic regression analysis was performed to create risk charts. Cardiac mortality was 10 and 22% for the sub-population of 2- and 5-year analyses. A four-parameter multivariate logistic regression model including age, New York Heart Association (NYHA) functional class, LVEF, and HMR was used. Annualized mortality rate was <1% in patients with NYHA Class I-II and HMR ≥ 2.0, irrespective of age and LVEF. In patients with NYHA Class III-IV, mortality rate was 4-6 times higher for HMR < 1.40 compared with HMR ≥ 2.0 in all LVEF classes. Among the subset of patients with b-type natriuretic peptide (BNP) results (n = 491 and 359 for 2- and 5-year models, respectively), the 5-year model showed incremental value of HMR in addition to BNP.
Both 2- and 5-year risk prediction models with (123)I-MIBG HMR can be used to identify low-risk as well as high-risk patients, which can be effective for further risk stratification of CHF patients even when BNP is available.
(123)I-间碘苄胍(MIBG)显像已广泛用于慢性心力衰竭(CHF)患者的预后评估。本研究的目的是创建用于预测心脏死亡短期(2年)和长期(5年)风险的死亡率风险图表。
利用1322例CHF患者的汇总数据库,进行多变量分析,包括(123)I-MIBG晚期心脏与纵隔比值(HMR)、左心室射血分数(LVEF)和临床因素,以确定使用患者子集(分别为n = 1280和933)预测2年和5年死亡风险的最佳变量。进行多变量逻辑回归分析以创建风险图表。2年和5年分析亚组的心脏死亡率分别为10%和22%。使用了一个包括年龄、纽约心脏协会(NYHA)功能分级、LVEF和HMR的四参数多变量逻辑回归模型。NYHA I-II级且HMR≥2.0的患者,无论年龄和LVEF如何,年化死亡率<1%。在NYHA III-IV级患者中,所有LVEF分级中,HMR<1.40的患者死亡率比HMR≥2.0的患者高4-6倍。在有B型利钠肽(BNP)结果的患者子集中(2年模型和5年模型分别为n = 491和359),5年模型显示除BNP外HMR具有增量价值。
(123)I-MIBG HMR的2年和5年风险预测模型均可用于识别低风险和高风险患者,即使在有BNP的情况下,这对于CHF患者的进一步风险分层也可能有效。