Lauridsen Marie Dam, Gammelager Henrik, Schmidt Morten, Rasmussen Thomas Bøjer, Shaw Richard E, Bøtker Hans Erik, Sørensen Henrik Toft, Christiansen Christian Fynbo
Department of Clinical Epidemiology, Aarhus University Hospital, Oluf Palmes Alle 43-45, 8200, Aarhus N, Denmark.
California Pacific Medical Institute Research Institute, 475 Brannan, Suite 220, San Francisco, CA, 94107, USA.
Crit Care. 2015 Dec 30;19:452. doi: 10.1186/s13054-015-1170-8.
Myocardial infarction-related cardiogenic shock is frequently complicated by acute kidney injury. We examined the influence of acute kidney injury treated with renal replacement therapy (AKI-RRT) on risk of chronic dialysis and mortality, and assessed the role of comorbidity in patients with cardiogenic shock.
In this Danish cohort study conducted during 2005-2012, we used population-based medical registries to identify patients diagnosed with first-time myocardial infarction-related cardiogenic shock and assessed their AKI-RRT status. We computed the in-hospital mortality risk and adjusted relative risk. For hospital survivors, we computed 5-year cumulative risk of chronic dialysis accounting for competing risk of death. Mortality after discharge was computed with use of Kaplan-Meier methods. We computed 5-year hazard ratios for chronic dialysis and death after discharge, comparing AKI-RRT with non-AKI-RRT patients using a propensity score-adjusted Cox regression model.
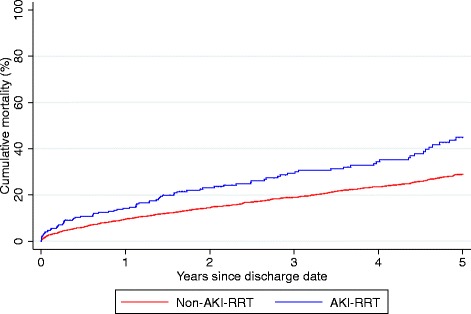
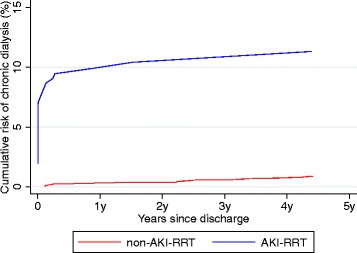
We identified 5079 patients with cardiogenic shock, among whom 13% had AKI-RRT. The in-hospital mortality was 62% for AKI-RRT patients, and 36% for non-AKI-RRT patients. AKI-RRT remained associated with increased in-hospital mortality after adjustment for confounders (relative risk=1.70, 95% confidence interval (CI): 1.59-1.81). Among the 3059 hospital survivors, the 5-year risk of chronic dialysis was 11% (95% CI: 8-16%) for AKI-RRT patients, and 1% (95% CI: 0.5-1%) for non-AKI-RRT patients (adjusted hazard ratio: 15.9 (95% CI: 8.7-29.3). The 5-year mortality was 43% (95% CI: 37-53%) for AKI-RRT patients compared with 29% (95% CI: 29-31%) for non-AKI-RRT patients. The adjusted 5-year hazard ratio for death was 1.55 (95% CI: 1.22-1.96) for AKI-RRT patients compared with non-AKI-RRT patients. In patients with comorbidity, absolute mortality increased while relative impact of AKI-RRT on mortality decreased.
AKI-RRT following myocardial infarction-related cardiogenic shock predicted elevated short-term mortality and long-term risk of chronic dialysis and mortality. The impact of AKI-RRT declined with increasing comorbidity suggesting that intensive treatment of AKI-RRT should be accompanied with optimized treatment of comorbidity when possible.
心肌梗死相关的心源性休克常并发急性肾损伤。我们研究了接受肾脏替代治疗的急性肾损伤(AKI-RRT)对慢性透析风险和死亡率的影响,并评估了合并症在患有心源性休克患者中的作用。
在这项于2005年至2012年期间进行的丹麦队列研究中,我们利用基于人群的医疗登记系统识别首次诊断为心肌梗死相关心源性休克的患者,并评估他们的AKI-RRT状态。我们计算了住院死亡率风险和调整后的相对风险。对于医院幸存者,我们计算了考虑死亡竞争风险后的5年慢性透析累积风险。出院后的死亡率采用Kaplan-Meier方法计算。我们使用倾向评分调整的Cox回归模型,比较AKI-RRT患者与非AKI-RRT患者,计算出院后慢性透析和死亡的5年风险比。
我们识别出5079例心源性休克患者,其中13%接受了AKI-RRT。AKI-RRT患者的住院死亡率为62%,非AKI-RRT患者为36%。在对混杂因素进行调整后,AKI-RRT仍然与住院死亡率增加相关(相对风险=1.70,95%置信区间(CI):1.59-1.81)。在3059例医院幸存者中,AKI-RRT患者的5年慢性透析风险为11%(95%CI:8-16%),非AKI-RRT患者为1%(95%CI:0.5-1%)(调整后的风险比:15.9(95%CI:8.7-29.3)。AKI-RRT患者的5年死亡率为43%(95%CI:37-53%),而非AKI-RRT患者为29%(95%CI:29-31%)。与非AKI-RRT患者相比,AKI-RRT患者调整后的5年死亡风险比为1.55(95%CI:1.22-1.96)。在合并症患者中,绝对死亡率增加,而AKI-RRT对死亡率的相对影响降低。
心肌梗死相关心源性休克后的AKI-RRT预示着短期死亡率升高以及慢性透析和死亡的长期风险增加。AKI-RRT的影响随着合并症的增加而下降,这表明在可能的情况下,对AKI-RRT进行强化治疗应同时对合并症进行优化治疗。