Malagola Michele, Skert Cristina, Borlenghi Erika, Chiarini Marco, Cattaneo Chiara, Morello Enrico, Cancelli Valeria, Cattina Federica, Cerqui Elisa, Pagani Chiara, Passi Angela, Ribolla Rossella, Bernardi Simona, Giustini Viviana, Lamorgese Cinzia, Ruggeri Giuseppina, Imberti Luisa, Caimi Luigi, Russo Domenico, Rossi Giuseppe
Unit of Blood Disease and Stem Cell Transplantation, Department of Clinical and Experimental Sciences, University of Brescia, AO Spedali Civili di Brescia, Brescia, Italy.
Division of Hematology, AO Spedali Civili di Brescia, Brescia, Italy.
Cancer Med. 2016 Feb;5(2):265-74. doi: 10.1002/cam4.593. Epub 2015 Dec 29.
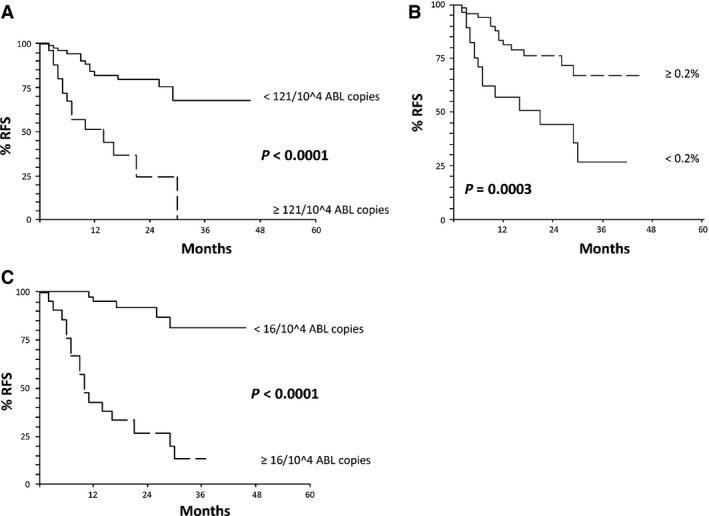
Risk stratification in acute myeloid leukemia (AML) patients using prognostic parameters at diagnosis is effective, but may be significantly improved by the use of on treatment parameters which better define the actual sensitivity to therapy in the single patient. Minimal residual disease (MRD) monitoring has been demonstrated crucial for the identification of AML patients at high risk of relapse, but the best method and timing of MRD detection are still discussed. Thus, we retrospectively analyzed 104 newly diagnosed AML patients, consecutively treated and monitored by quantitative polymerase chain reactions (Q-PCR) on WT1 and by multiparametric flow cytometry (MFC) on leukemia-associated immunophenotypes (LAIPs) at baseline, after induction, after 1st consolidation and after 1st intensification. By multivariate analysis, the factors independently associated with adverse relapse-free survival (RFS) were: bone marrow (BM)-WT1 ≥ 121/10(4) ABL copies (P = 0.02) and LAIP ≥ 0.2% (P = 0.0001) (after 1st consolidation) (RFS at the median follow up of 12.5 months: 51% vs. 82% [P < 0.0001] and 57% vs. 81%, respectively [P = 0.0003]) and PB-WT1 ≥ 16/10(4) ABL copies (P = 0.0001) (after 1st intensification) (RFS 43% vs. 95% [P < 0.0001]) Our data confirm the benefits of sequential MRD monitoring with both Q-PCR and MFC. If confirmed by further prospective trials, they may significantly improve the possibility of a risk-adapted, postinduction therapy of AML.
利用诊断时的预后参数对急性髓系白血病(AML)患者进行风险分层是有效的,但通过使用能更好地确定单个患者实际治疗敏感性的治疗过程中的参数,风险分层可能会得到显著改善。微小残留病(MRD)监测已被证明对于识别有高复发风险的AML患者至关重要,但MRD检测的最佳方法和时机仍在讨论中。因此,我们回顾性分析了104例新诊断的AML患者,这些患者在基线、诱导后、首次巩固后和首次强化后连续接受治疗,并通过对WT1进行定量聚合酶链反应(Q-PCR)以及对白血病相关免疫表型(LAIPs)进行多参数流式细胞术(MFC)监测。通过多变量分析,与无复发生存期(RFS)不良独立相关的因素为:骨髓(BM)-WT1≥121/10(4) ABL拷贝数(P = 0.02)和LAIP≥0.2%(P = 0.0001)(首次巩固后)(中位随访12.5个月时的RFS:分别为51% vs. 82% [P < 0.0001]和57% vs. 81% [P = 0.0003])以及外周血(PB)-WT1≥16/10(4) ABL拷贝数(P = 0.0001)(首次强化后)(RFS为43% vs. 95% [P < 0.0001])。我们的数据证实了采用Q-PCR和MFC进行序贯MRD监测的益处。如果能得到进一步前瞻性试验的证实,这些数据可能会显著提高AML诱导后进行风险适应性治疗的可能性。