Koch Anne Mette, Nilsen Roy Miodini, Eriksen Hanne Merete, Cox Rebecca Jane, Harthug Stig
Department of Research and Development, Haukeland University Hospital, Jonas Liesv. 65, 5021 Bergen, Norway ; Department of Clinical Science, University of Bergen, Jonas Liesv. 87, Bergen, Norway.
Department of Research and Development, Haukeland University Hospital, Jonas Liesv. 65, 5021 Bergen, Norway.
Antimicrob Resist Infect Control. 2015 Dec 29;4:57. doi: 10.1186/s13756-015-0097-9. eCollection 2015.
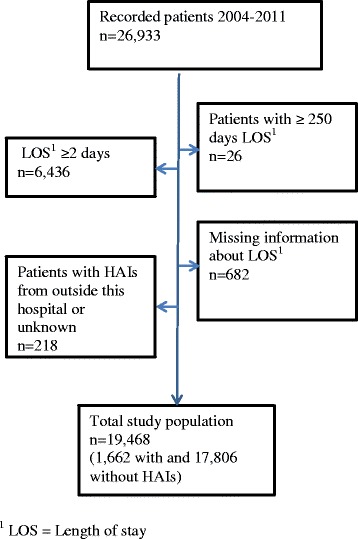
Hospital-associated infections (HAIs) are reported to increase patient mortality and incur longer hospital stays. Most studies to date have focused on specific groups of hospitalised patients with a rather short follow-up period. In this repeated cross-sectional study, with prospective follow-up of 19,468 hospitalized patients, we aimed to analyze the impact of HAIs on mortality 30 days and 1 year after the prevalence survey date.
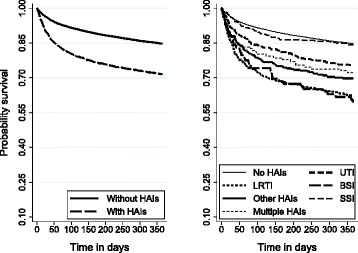
The study was conducted at Haukeland University Hospital, Norway, a large combined emergency and referral teaching hospital, from 2004 to 2011 with follow-up until November 2012. Prevalence of all types of HAIs including urinary tract infections (UTI), lower respiratory tract infections (LRTI), surgical site infections (SSI) and blood stream infections (BSI) were recorded four times every year. Information on the date of birth, admission and discharge from the hospital, number of diagnoses (ICD-10 codes) and patient's mortality was retrieved from the patient administrative data system. The data were analysed by Kaplan-Meier survival analysis and by multiple Cox regression analysis, adjusted for year of registration, time period, sex, type of admission, Charlson comorbidity index, surgical operation, use of urinary tract catheter and time from admission to the prevalence survey date.
The overall prevalence of HAIs was 8.5 % (95 % CI: 8.1, 8.9). Patients with HAIs had an adjusted hazard ratio (HR) of 1.5 (95 % CI: 1.3, 1.8,) and 1.4 (95 % CI: 1.2, 1.5) for death within 30-days and 1 year, relative to those without HAIs. Subgroup analyses revealed that patients with BSI, LRTI or more than one simultaneous infection had an increased risk of death.
In this long time follow-up study, we found that HAIs have severe consequences for the patients. BSI, LRTI and more than one simultaneous infection were independently and strongly associated with increased mortality 30 days and 1 year after inclusion in the study.
据报道,医院感染(HAIs)会增加患者死亡率并延长住院时间。迄今为止,大多数研究都集中在特定住院患者群体,且随访期较短。在这项针对19468名住院患者进行前瞻性随访的重复横断面研究中,我们旨在分析医院感染对患病率调查日期后30天和1年死亡率的影响。
该研究于2004年至2011年在挪威哈肯兰大学医院进行,这是一家大型综合急诊和转诊教学医院,随访至2012年11月。每年记录包括尿路感染(UTI)、下呼吸道感染(LRTI)、手术部位感染(SSI)和血流感染(BSI)在内的所有类型医院感染的患病率。从患者管理数据系统中获取出生日期、入院和出院日期、诊断数量(ICD - 10编码)以及患者死亡率等信息。数据通过Kaplan - Meier生存分析和多元Cox回归分析进行分析,并根据登记年份、时间段、性别、入院类型、Charlson合并症指数、手术操作、尿路导管使用情况以及从入院到患病率调查日期的时间进行调整。
医院感染的总体患病率为8.5%(95%置信区间:8.1,8.9)。与未发生医院感染的患者相比,发生医院感染的患者在30天内和1年内死亡的调整后风险比(HR)分别为1.5(95%置信区间:1.3,1.8)和1.4(95%置信区间:1.2,1.5)。亚组分析显示,发生血流感染、下呼吸道感染或同时发生多种感染的患者死亡风险增加。
在这项长期随访研究中,我们发现医院感染对患者有严重影响。在纳入研究后30天和1年,血流感染、下呼吸道感染以及同时发生多种感染与死亡率增加独立且密切相关。