Tomini F, Prinzen F, van Asselt A D I
Department of Clinical Epidemiology and Medical Technology Assessment, Maastricht University Medical Centre, Maastricht, The Netherlands.
Department of Physiology, Cardiovascular Research Institute Maastricht (CARIM), Maastricht, The Netherlands.
Eur J Health Econ. 2016 Dec;17(9):1159-1172. doi: 10.1007/s10198-015-0752-3. Epub 2016 Jan 4.
Cardiac resynchronization therapy with a biventricular pacemaker (CRT-P) is an effective treatment for dyssynchronous heart failure (DHF). Adding an implantable cardioverter defibrillator (CRT-D) may further reduce the risk of sudden cardiac death (SCD). However, if the majority of patients do not require shock therapy, the cost-effectiveness ratio of CRT-D compared to CRT-P may be high. The objective of this study was to systematically review decision models evaluating the cost-effectiveness of CRT-D for patients with DHF, compare the structure and inputs of these models and identify the main factors influencing the ICERs for CRT-D.
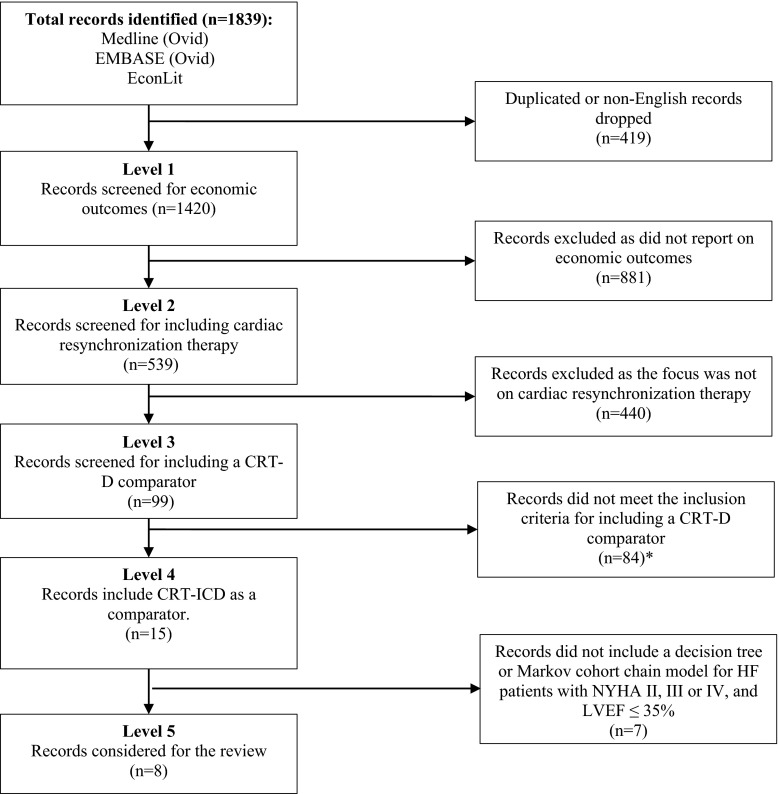
A comprehensive search strategy of Medline (Ovid), Embase (Ovid) and EconLit identified eight cost-effectiveness models evaluating CRT-D against optimal pharmacological therapy (OPT) and/or CRT-P.
The selected economic studies differed in terms of model structure, treatment path, time horizons, and sources of efficacy data. CRT-D was found cost-effective when compared to OPT but its cost-effectiveness became questionable when compared to CRT-P.
Cost-effectiveness of CRT-D may increase depending on improvement of all-cause mortality rates and HF mortality rates in patients who receive CRT-D, costs of the device, and battery life. In particular, future studies need to investigate longer-term mortality rates and identify CRT-P patients that will gain the most, in terms of life expectancy, from being treated with a CRT-D.
双心室起搏器心脏再同步治疗(CRT-P)是治疗不同步心力衰竭(DHF)的有效方法。增加植入式心律转复除颤器(CRT-D)可能会进一步降低心源性猝死(SCD)风险。然而,如果大多数患者不需要电击治疗,与CRT-P相比,CRT-D的成本效益比可能较高。本研究的目的是系统评价评估CRT-D治疗DHF患者成本效益的决策模型,比较这些模型的结构和输入,并确定影响CRT-D增量成本效果比(ICER)的主要因素。
通过对Medline(Ovid)、Embase(Ovid)和EconLit进行全面检索策略,确定了8个评估CRT-D与最佳药物治疗(OPT)和/或CRT-P对比的成本效益模型。
所选的经济学研究在模型结构、治疗路径、时间范围和疗效数据来源方面存在差异。与OPT相比,CRT-D具有成本效益,但与CRT-P相比,其成本效益受到质疑。
CRT-D的成本效益可能会随着接受CRT-D治疗患者的全因死亡率和心力衰竭死亡率的改善、设备成本以及电池寿命而增加。特别是,未来的研究需要调查长期死亡率,并确定在预期寿命方面从CRT-D治疗中获益最大的CRT-P患者。