O'Donoghue Michelle L, Bhatt Deepak L, Stone Gregg W, Steg Ph Gabriel, Gibson C Michael, Hamm Christian W, Price Matthew J, Prats Jayne, Liu Tiepu, Deliargyris Efthymios N, Mahaffey Kenneth W, White Harvey D, Harrington Robert A
From Cardiovascular Division, Brigham and Women's Hospital, Boston, MA (M.L.O., D.L.B.); Columbia University Medical Center and the Cardiovascular Research Foundation, New York, NY (G.W.S.); FACT, DHU FIRE, Université Paris-Diderot, Sorbonne Paris-Cité, France (G.S.); LVTS INSERM U-1148, Hôpital Bichat, HUPNVS, AP-HP, Paris, France (G.S.); NHLI, Imperial College, Royal Brompton Hospital, London, United Kingdom (G.S.); Beth Israel Deaconess Medical Center, Division of Cardiology, Boston, MA (C.M.G.); Kerckhoff Heart and Thorax Center, Bad Nauheim, Germany (C.W.H.); Scripps Clinic and Scripps Translational Science Institute, La Jolla, CA (M.J.P.); The Medicines Company, Parsippany, NJ (J.P., T.L., E.N.D.); Stanford University Medical School, Stanford, CA (K.W.M., R.A.H.); and Green Lane Cardiovascular Service, Auckland, New Zealand (H.D.W.).
Circulation. 2016 Jan 19;133(3):248-55. doi: 10.1161/CIRCULATIONAHA.115.017300.
Cangrelor is an intravenous ADP receptor antagonist that leads to potent and reversible inhibition of platelet aggregation. The relative safety and efficacy of some antiplatelet drugs in women has been disputed.
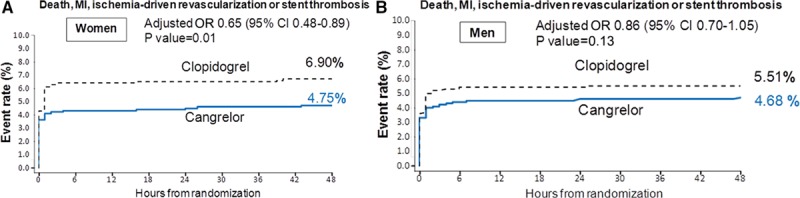
The Cangrelor versus Standard Therapy to Achieve Optimal Management of Platelet Inhibition (CHAMPION PHOENIX) trial randomized 11,145 patients undergoing elective or urgent percutaneous coronary intervention to cangrelor or clopidogrel. The primary efficacy end point was the composite of death, myocardial infarction, ischemia-driven revascularization, or stent thrombosis at 48 hours; the key secondary end point was stent thrombosis at 48 hours. The primary safety end point was GUSTO severe bleeding at 48 hours. Of subjects analyzed, 3051 (28%) were female. Cangrelor reduced the odds of the primary end point by 35% in women (adjusted odds ratio [OR], 0.65; 95% confidence interval [CI], 0.48-0.89) and by 14% in men (OR, 0.86; 95% CI, 0.70-1.05; P interaction=0.23) compared with clopidogrel. Cangrelor reduced the odds of stent thrombosis by 61% in women (OR, 0.39; 95% CI, 0.20-0.77) and 16% in men (OR, 0.84; 95% CI, 0.53-1.33; P interaction=0.11). The odds of severe bleeding were similar in both women and men treated with cangrelor (0.3% versus 0.2%, P=0.30 [women]; 0.1% versus 0.1%, P=0.41 [men]; P interaction=0.88) versus clopidogrel. Cangrelor increased the odds of moderate bleeding in women (0.9% versus 0.3%, P=0.02), but not in men (0.2% versus 0.2%, P=0.68; P interaction=0.040). The net clinical benefit (primary efficacy and safety end point) favored cangrelor in both women (OR, 0.68; 95% CI, 0.50-0.92) and men (OR, 0.87; 95% CI, 0.71-1.06; P interaction=0.26).
In CHAMPION PHOENIX, cangrelor reduced the odds of major adverse cardiovascular events and stent thrombosis in women and men and appeared to offer greater net clinical benefit than clopidogrel.
URL: http://www.clinicaltrials.gov. Unique identifier: NCT01156571.
坎格雷洛是一种静脉注射的ADP受体拮抗剂,可有效且可逆地抑制血小板聚集。一些抗血小板药物在女性中的相对安全性和疗效一直存在争议。
坎格雷洛与标准疗法以实现血小板抑制的最佳管理(CHAMPION PHOENIX)试验将11145例接受择期或紧急经皮冠状动脉介入治疗的患者随机分为接受坎格雷洛或氯吡格雷治疗。主要疗效终点是48小时时死亡、心肌梗死、缺血驱动的血运重建或支架血栓形成的复合终点;关键次要终点是48小时时的支架血栓形成。主要安全终点是48小时时的GUSTO严重出血。在分析的受试者中,3051例(28%)为女性。与氯吡格雷相比,坎格雷洛使女性主要终点事件的发生率降低35%(调整后的优势比[OR]为0.65;95%置信区间[CI]为0.48 - 0.89),男性降低14%(OR为0.86;95%CI为0.70 - 1.05;P交互作用 = 0.23)。坎格雷洛使女性支架血栓形成的发生率降低61%(OR为0.39;95%CI为0.20 - 0.77),男性降低16%(OR为0.84;95%CI为0.53 - 1.33;P交互作用 = 0.11)。接受坎格雷洛治疗的女性和男性严重出血的发生率相似(0.3%对0.2%,P = 0.30[女性];0.1%对0.1%,P = 0.41[男性];P交互作用 = 0.88)与氯吡格雷相比。坎格雷洛增加了女性中度出血的发生率(0.9%对0.3%,P = 0.02),但男性未增加(0.2%对0.2%,P = 0.68;P交互作用 = 0.040)。净临床获益(主要疗效和安全终点)在女性(OR为0.68;95%CI为0.50 - 0.92)和男性(OR为0.87;95%CI为0.71 - 1.06;P交互作用 = 0.26)中均有利于坎格雷洛。
在CHAMPION PHOENIX试验中,坎格雷洛降低了女性和男性主要不良心血管事件和支架血栓形成的发生率,并且似乎比氯吡格雷提供了更大的净临床获益。