Suzuki Kodai, Inoue Shigeaki, Morita Seiji, Watanabe Nobuo, Shintani Ayumi, Inokuchi Sadaki, Ogura Shinji
Department of Emergency and Disaster Medicine, Gifu University Graduate School of Medicine, Gifu, Japan.
Department of Emergency and Critical Care Medicine, Tokai University School of Medicine, Isehara, Kanagawa, Japan.
PLoS One. 2016 Jan 14;11(1):e0145963. doi: 10.1371/journal.pone.0145963. eCollection 2016.
Although emergency resuscitative thoracotomy is performed as a salvage maneuver for critical blunt trauma patients, evidence supporting superior effectiveness of emergency resuscitative thoracotomy compared to conventional closed-chest compressions remains insufficient. The objective of this study was to investigate whether emergency resuscitative thoracotomy at the emergency department or in the operating room was associated with favourable outcomes after blunt trauma and to compare its effectiveness with that of closed-chest compressions.
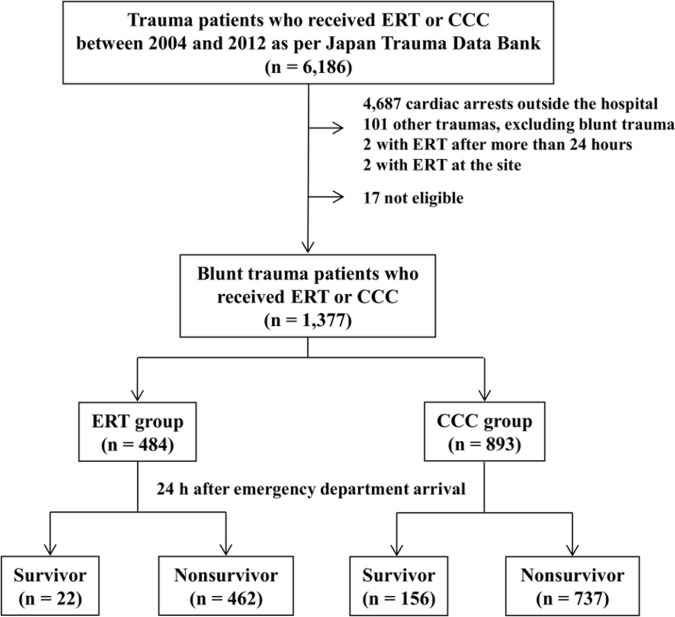
This was a retrospective nationwide cohort study. Data were obtained from the Japan Trauma Data Bank for the period between 2004 and 2012. The primary and secondary outcomes were patient survival rates 24 h and 28 d after emergency department arrival. Statistical analyses were performed using multivariable generalized mixed-effects regression analysis. We adjusted for the effects of different hospitals by introducing random intercepts in regression analysis to account for the differential quality of emergency resuscitative thoracotomy at hospitals where patients in cardiac arrest were treated. Sensitivity analyses were performed using propensity score matching.
In total, 1,377 consecutive, critical blunt trauma patients who received cardiopulmonary resuscitation in the emergency department or operating room were included in the study. Of these patients, 484 (35.1%) underwent emergency resuscitative thoracotomy and 893 (64.9%) received closed-chest compressions. Compared to closed-chest compressions, emergency resuscitative thoracotomy was associated with lower survival rate 24 h after emergency department arrival (4.5% vs. 17.5%, respectively, P < 0.001) and 28 d after arrival (1.2% vs. 6.0%, respectively, P < 0.001). Multivariable generalized mixed-effects regression analysis with and without a propensity score-matched dataset revealed that the odds ratio for an unfavorable survival rate after 24 h was lower for emergency resuscitative thoracotomy than for closed-chest compressions (P < 0.001).
Emergency resuscitative thoracotomy was independently associated with decreased odds of a favorable survival rate compared to closed-chest compressions.
尽管急诊复苏性开胸手术是作为抢救严重钝性创伤患者的一种挽救措施,但与传统的胸外按压相比,支持急诊复苏性开胸手术具有更高有效性的证据仍然不足。本研究的目的是调查在急诊科或手术室进行的急诊复苏性开胸手术与钝性创伤后良好结局是否相关,并将其有效性与胸外按压进行比较。
这是一项全国性的回顾性队列研究。数据来自日本创伤数据库2004年至2012年期间的数据。主要和次要结局是患者到达急诊科后24小时和28天的生存率。使用多变量广义混合效应回归分析进行统计分析。我们在回归分析中引入随机截距来调整不同医院的影响,以考虑在进行心脏骤停患者治疗的医院中急诊复苏性开胸手术的质量差异。使用倾向得分匹配进行敏感性分析。
本研究共纳入了1377例在急诊科或手术室接受心肺复苏的连续严重钝性创伤患者。其中,484例(35.1%)接受了急诊复苏性开胸手术,893例(64.9%)接受了胸外按压。与胸外按压相比,急诊复苏性开胸手术与患者到达急诊科后24小时的生存率较低相关(分别为4.5%和17.5%,P<0.001)以及到达后28天的生存率较低相关(分别为1.2%和6.0%,P<0.001)。使用和不使用倾向得分匹配数据集的多变量广义混合效应回归分析显示,急诊复苏性开胸手术24小时后不良生存率的优势比低于胸外按压(P<0.001)。
与胸外按压相比,急诊复苏性开胸手术独立地与良好生存率的几率降低相关。