Dubrovskaya Yanina, Tejada Rainer, Bosco Joseph, Stachel Anna, Chen Donald, Feng Melinda, Rosenberg Andrew, Phillips Michael
Department of Pharmacy, NYU Langone Medical Center, New York, NY, USA.
Department of Infection Prevention and Control, NYU Langone Medical Center, New York, NY, USA.
SAGE Open Med. 2015 Oct 28;3:2050312115612803. doi: 10.1177/2050312115612803. eCollection 2015.
Recent studies described an increase in acute kidney injury when high dose gentamicin was included in perioperative prophylaxis for orthopedic surgeries. To this effect, we compared the rate of nephrotoxicity for selected orthopedic surgeries where gentamicin was included (Gentamicin Group) to those where it was not included (Control Group) for perioperative prophylaxis and evaluated risk factors for nephrotoxicity.
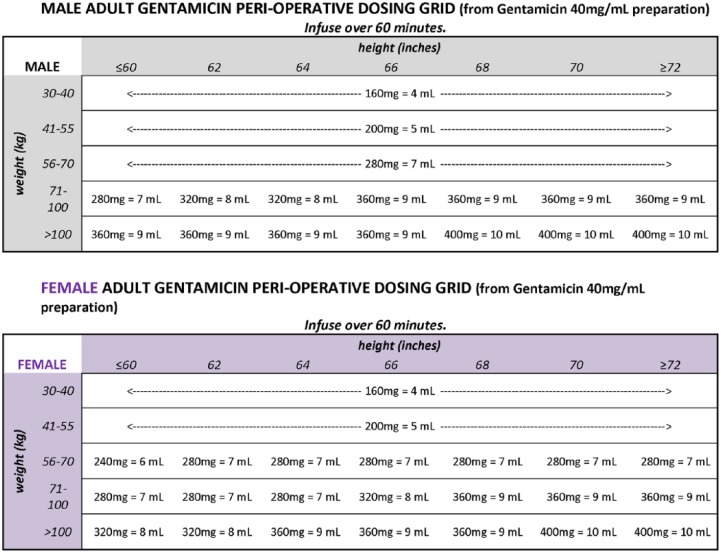
Spine, hip and knee surgeries performed between April 2011 and December 2013 were reviewed retrospectively. Gentamicin was given to eligible patients based on age, weight and Creatinine Clearance. Nephrotoxicity was assessed using Risk, Injury, Failure, Loss, End-stage kidney disease (RIFLE) criteria.
Among selected surgeries (N = 1590 in Gentamicin Group: hip = 926, spine = 600, knee = 64; N = 2587 in
hip = 980, spine = 902, knee = 705), patients' body weight, serum creatinine, comorbidities and surgery duration were similar in Gentamicin Group and CONTROL GROUP. Gentamicin median dose was 4.5 mg/kg of dosing weight. Nephrotoxicity rate was 2.5% in Gentamicin Group and 1.8% in CONTROL GROUP, p = 0.17. Most cases of nephrotoxicity were Risk category by RIFLE criteria (67% in Gentamicin Group and 72% in CONTROL GROUP, p = 0.49). In logistic regression, risk factors for nephrotoxicity were hospital stay >1 day prior to surgery (odds ratio = 8.1; 95% confidence interval = 2.25-28.97, p = 0.001), knee or hip surgery (odds ratio = 4.7; 95% confidence interval = 2.9-9.48, p = 0.0005) and diabetes (odds ratio = 1.95; 95% confidence interval = 1.13-3.35, p = 0.016). Receipt of gentamicin was not an independent predictor of nephrotoxicity (odds ratio = 1.5; 95% confidence interval = 0.97-2.35, p = 0.07).
In this cohort, rate of nephrotoxicity was similar between Gentamicin Group and Control Group. Single high dose gentamicin is a safe and acceptable option for perioperative prophylaxis in eligible patients undergoing orthopedic surgeries.
近期研究表明,在骨科手术围手术期预防用药中使用高剂量庆大霉素时,急性肾损伤的发生率会增加。为此,我们比较了在围手术期预防用药中使用庆大霉素的特定骨科手术(庆大霉素组)与未使用庆大霉素的手术(对照组)的肾毒性发生率,并评估了肾毒性的危险因素。
回顾性分析2011年4月至2013年12月期间进行的脊柱、髋关节和膝关节手术。根据年龄、体重和肌酐清除率给符合条件的患者使用庆大霉素。使用风险、损伤、衰竭、丧失、终末期肾病(RIFLE)标准评估肾毒性。
在选定的手术中(庆大霉素组N = 1590:髋关节手术 = 926例,脊柱手术 = 600例,膝关节手术 = 64例;对照组N = 2587:髋关节手术 = 980例,脊柱手术 = 902例,膝关节手术 = 705例),庆大霉素组和对照组患者的体重、血清肌酐、合并症和手术持续时间相似。庆大霉素的中位剂量为4.5 mg/kg给药体重。庆大霉素组的肾毒性发生率为2.5%,对照组为1.8%,p = 0.17。根据RIFLE标准,大多数肾毒性病例为风险类别(庆大霉素组为67%,对照组为72%,p = 0.49)。在逻辑回归中,肾毒性的危险因素为术前住院时间>1天(比值比 = 8.1;95%置信区间 = 2.25 - 28.97,p = 0.001)、膝关节或髋关节手术(比值比 = 4.7;95%置信区间 = 至2.9 - 9.48,p = 0.0005)和糖尿病(比值比 = 1.95;95%置信区间 = 1.13 - 3.35,p = 0.016)。接受庆大霉素并非肾毒性的独立预测因素(比值比 = 1.5;95%置信区间 = 0.97 - 2.35,p = 0.07)。
在该队列中,庆大霉素组和对照组的肾毒性发生率相似。对于接受骨科手术的符合条件的患者,单次高剂量庆大霉素是围手术期预防用药的一种安全且可接受的选择。