Ye Zi, Austin Erin, Schaid Daniel J, Kullo Iftikhar J
Division of Cardiovascular Diseases and the Gonda Vascular Center, Mayo Clinic, Rochester, MN, USA.
Division of Cardiovascular Diseases and the Gonda Vascular Center, Mayo Clinic, Rochester, MN, USA; Department of Health Science Research, Mayo Clinic, Rochester, MN, USA.
Atherosclerosis. 2016 Mar;246:274-9. doi: 10.1016/j.atherosclerosis.2015.12.031. Epub 2016 Jan 5.
We investigated whether a multi-locus genetic risk scores (GRS) was associated with presence and progression of abdominal aortic aneurysm (AAA) in a case - control study.
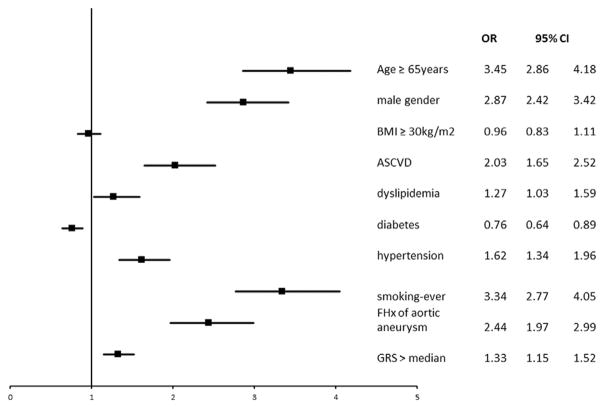
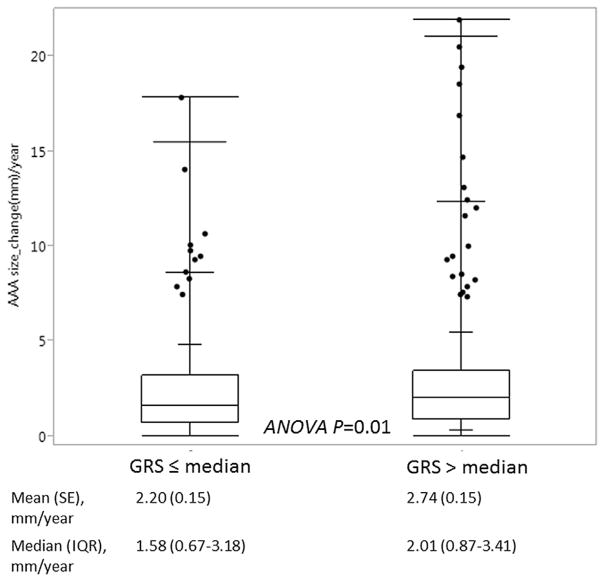
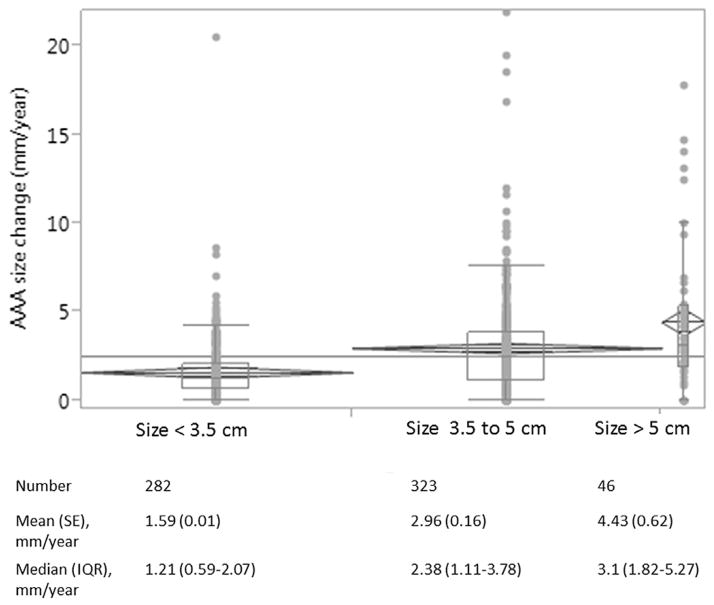
The study comprised of 1124 patients with AAA (74 ± 8 years, 83% men, 52% of them with a maximal AAA size ≤ 5 cm) and 6524 non-cases (67 ± 11 years, 58% men) from the Mayo Vascular Disease Biorepository. AAA was defined as infrarenal abdominal aorta diameter ≥ 3.0 cm or history of AAA repair. Non-cases were participants without known AAA. A GRS was calculated using 4 SNPs associated with AAA at genome-wide significance (P ≤ 10(-8)). The GRS was associated with the presence of AAA after adjustment for age, sex, cardiovascular risk factors, atherosclerotic cardiovascular diseases and family history of aortic aneurysm: odds ratio (OR, 95% confidence interval, CI) 1.06 (1.04-1.09, p < 0.001). Adding GRS to conventional risk factors improved the association of presence of AAA (net reclassification index 14%, p < 0.001). In a subset of patients with AAA who had ≥ 2 imaging studies (n = 651, mean (SE) growth rate 2.47 (0.11) mm/year during a mean time interval of 5.41 years), GRS, baseline size, diabetes and family history were each associated with aneurysm growth rate in univariate association (all p < 0.05). The estimated mean aneurysm growth rate was 0.50 mm/year higher in those with GRS > median (5.78) than those with GRS ≤ median (p = 0.01), after adjustment for baseline size (p < 0.001), diabetes (p = 0.046) and family history of aortic aneurysm (p = 0.02).
A multi-locus GRS was associated with presence of AAA and greater aneurysm expansion.
在一项病例对照研究中,我们调查了多基因座遗传风险评分(GRS)是否与腹主动脉瘤(AAA)的发生及进展相关。
该研究纳入了梅奥血管疾病生物样本库中的1124例AAA患者(74±8岁,83%为男性,其中52%的AAA最大直径≤5 cm)和6524例非病例(67±11岁,58%为男性)。AAA定义为肾下腹主动脉直径≥3.0 cm或有AAA修复史。非病例为无已知AAA的参与者。使用4个在全基因组水平具有显著意义(P≤10⁻⁸)的与AAA相关的单核苷酸多态性(SNP)计算GRS。在调整年龄、性别、心血管危险因素、动脉粥样硬化性心血管疾病和主动脉瘤家族史后,GRS与AAA的发生相关:比值比(OR,95%置信区间,CI)为1.06(1.04 - 1.09,p<0.001)。将GRS添加到传统危险因素中可改善AAA存在情况的关联性(净重新分类指数为14%,p<0.001)。在一组有≥2次影像学检查的AAA患者亚组(n = 651,在平均时间间隔5.41年期间平均(标准误)生长速率为2.47(0.11)mm/年)中,GRS、基线大小、糖尿病和家族史在单变量关联中均与动脉瘤生长速率相关(所有p<0.05)。在调整基线大小(p<0.001)、糖尿病(p = 0.046)和主动脉瘤家族史(p = 0.02)后,GRS>中位数(5.78)者的估计平均动脉瘤生长速率比GRS≤中位数者高0.50 mm/年(p = 0.01)。
多基因座GRS与AAA的存在及更大的动脉瘤扩张相关。