Barbui Corrado, Bighelli Irene, Carrà Giuseppe, Castellazzi Mariasole, Lucii Claudio, Martinotti Giovanni, Nosè Michela, Ostuzzi Giovanni
WHO Collaborating Centre for Research and Training in Mental Health and Service Evaluation, Section of Psychiatry, University of Verona, Verona, Italy.
Division of Psychiatry, University College of London, UK, and Department of Medicine and Surgery, University of Milano Bicocca, Milan, Italy.
PLoS One. 2016 Feb 3;11(2):e0148212. doi: 10.1371/journal.pone.0148212. eCollection 2016.
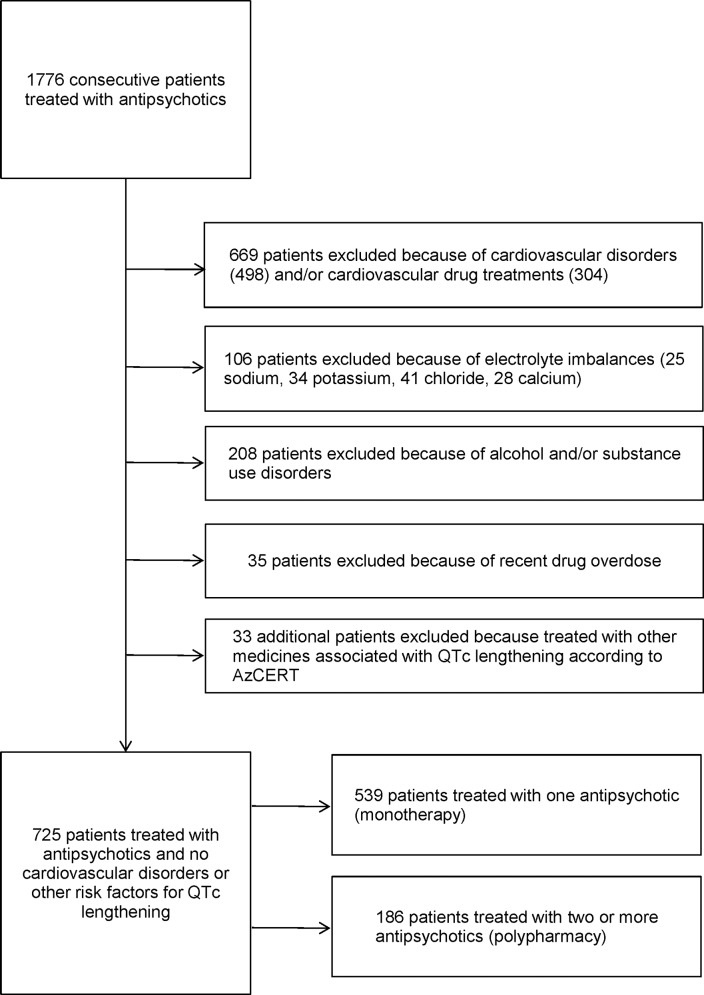
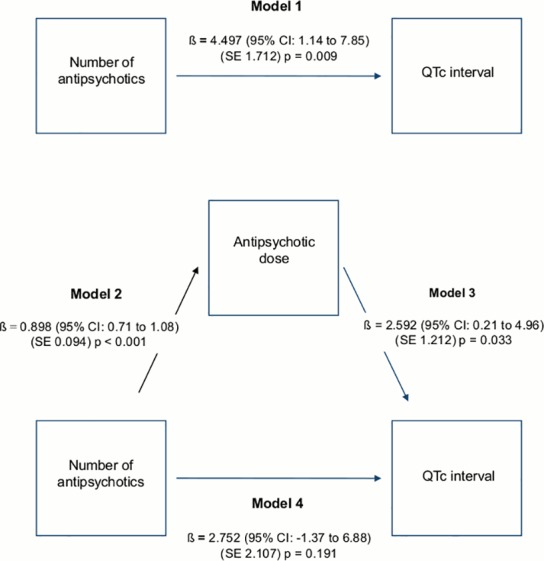
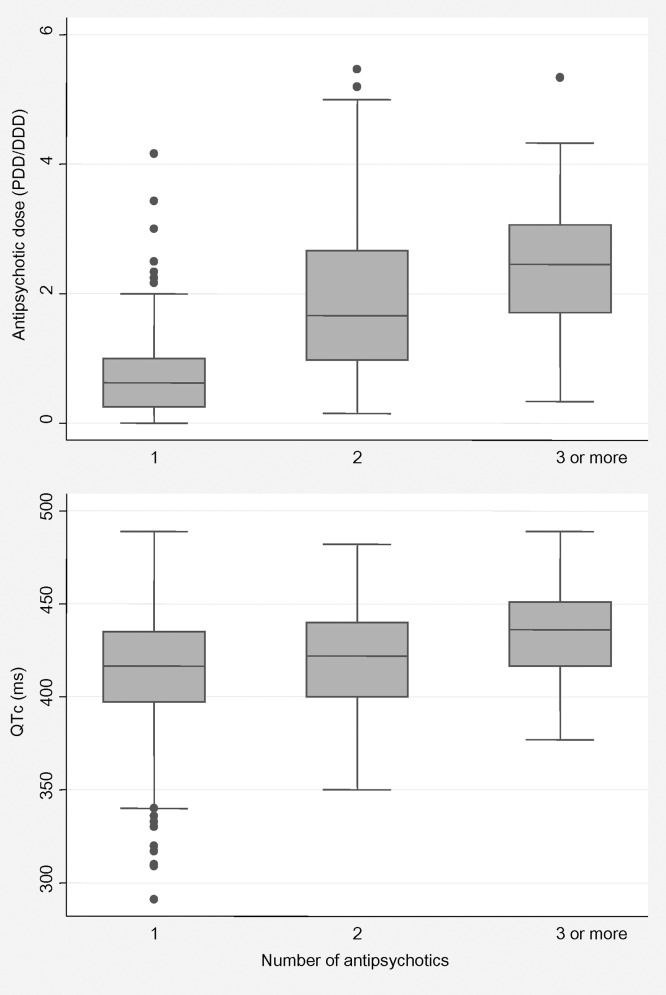
Antipsychotic (AP) drugs have the potential to cause prolongation of the QT interval corrected for heart rate (QTc). As this risk is dose-dependent, it may be associated with the number of AP drugs concurrently prescribed, which is known to be associated with increased cumulative equivalent AP dosage. This study analysed whether AP dose mediates the relationship between polypharmacy and QTc interval. We used data from a cross-sectional survey that investigated the prevalence of QTc lengthening among people with psychiatric illnesses in Italy. AP polypharmacy was tested for evidence of association with AP dose and QTc interval using the Baron and Kenny mediational model. A total of 725 patients were included in this analysis. Of these, 186 (26%) were treated with two or more AP drugs (AP polypharmacy). The mean cumulative AP dose was significantly higher in those receiving AP polypharmacy (prescribed daily dose/defined daily dose = 2.93, standard deviation 1.31) than monotherapy (prescribed daily dose/defined daily dose = 0.82, standard deviation 0.77) (z = -12.62, p < 0.001). Similarly, the mean QTc interval was significantly longer in those receiving AP polypharmacy (mean = 420.86 milliseconds, standard deviation 27.16) than monotherapy (mean = 413.42 milliseconds, standard deviation 31.54) (z = -2.70, p = 0.006). The Baron and Kenny mediational analysis showed that, after adjustment for confounding variables, AP dose mediates the association between polypharmacy and QTc interval. The present study found that AP polypharmacy is associated with QTc interval, and this effect is mediated by AP dose. Given the high prevalence of AP polypharmacy in real-world clinical practice, clinicians should consider not only the myriad risk factors for QTc prolongation in their patients, but also that adding a second AP drug may further increase risk as compared with monotherapy.
抗精神病药物(AP)有延长经心率校正的QT间期(QTc)的潜在风险。由于这种风险具有剂量依赖性,它可能与同时开具的AP药物数量有关,而这又与累积等效AP剂量增加相关。本研究分析了AP剂量是否介导了联合用药与QTc间期之间的关系。我们使用了一项横断面调查的数据,该调查研究了意大利精神疾病患者中QTc延长的患病率。使用Baron和Kenny中介模型检验了AP联合用药与AP剂量和QTc间期之间的关联证据。本分析共纳入725例患者。其中,186例(26%)接受了两种或更多种AP药物治疗(AP联合用药)。接受AP联合用药的患者的平均累积AP剂量(规定日剂量/限定日剂量 = 2.93,标准差1.31)显著高于单药治疗患者(规定日剂量/限定日剂量 = 0.82,标准差0.77)(z = -12.62,p < 0.001)。同样,接受AP联合用药的患者的平均QTc间期(均值 = 420.86毫秒,标准差27.16)显著长于单药治疗患者(均值 = 413.42毫秒,标准差31.54)(z = -2.70,p = 0.006)。Baron和Kenny中介分析表明,在对混杂变量进行校正后,AP剂量介导了联合用药与QTc间期之间的关联。本研究发现,AP联合用药与QTc间期相关,且这种效应由AP剂量介导。鉴于在实际临床实践中AP联合用药的高患病率,临床医生不仅应考虑患者中QTc延长的众多危险因素,还应考虑与单药治疗相比,添加第二种AP药物可能会进一步增加风险。