Kim Wonhee, Lee Yoonje, Kim Changsun, Lim Tae Ho, Oh Jaehoon, Kang Hyunggoo, Lee Sanghyun
From the Department of Emergency Medicine, Kangnam Sacred Heart Hospital, Hallym University, Republic of Korea (WK); Department of Emergency Medicine, Guri Hospital, Hanyang University, Republic of Korea (YL, CK); and Department of Emergency Medicine, Seoul Hospital, Hanyang University, Republic of Korea (THL, JO, HK, SL).
Medicine (Baltimore). 2016 Feb;95(5):e2631. doi: 10.1097/MD.0000000000002631.
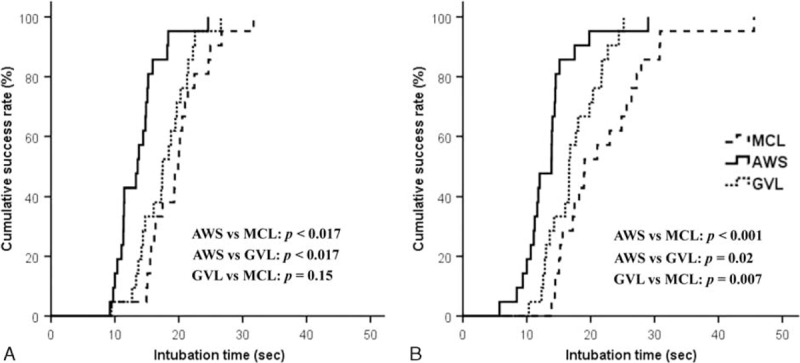
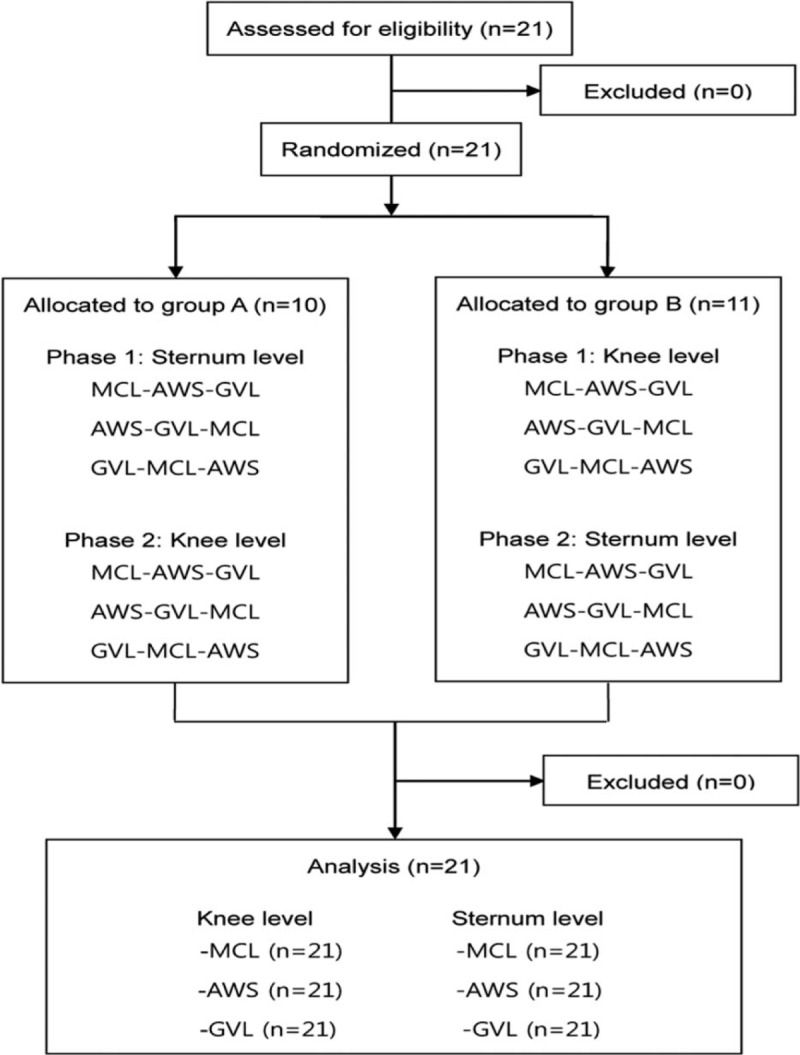
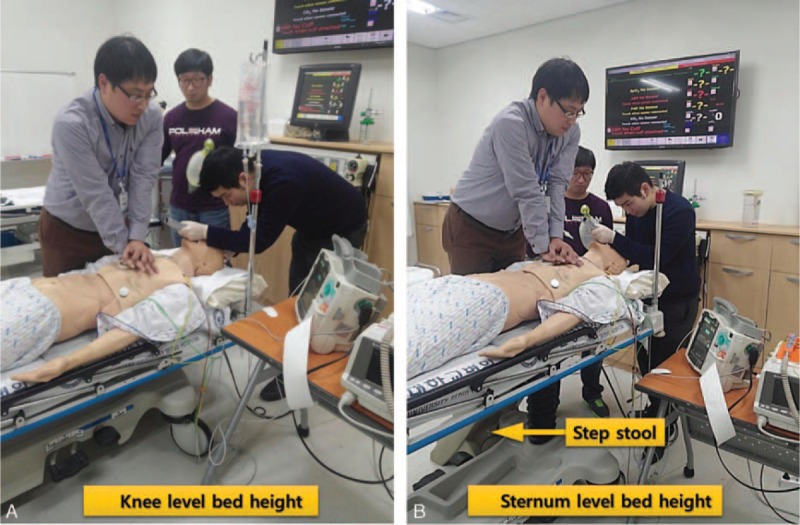
We aimed to investigate whether bed height affects intubation performance in the setting of cardiopulmonary resuscitation and which type of laryngoscope shows the best performance at each bed height.A randomized crossover manikin study was conducted. Twenty-one participants were enrolled, and they were randomly allocated to 2 groups: group A (n = 10) and group B (n = 11). The participants underwent emergency endotracheal intubation (ETI) using the Airwayscope (AWS), Glidescope video laryngoscope, and Macintosh laryngoscope in random order while chest compression was performed. Each ETI was conducted at 2 levels of bed height (minimum bed height: 68.9 cm and maximum bed height: 101.3 cm). The primary outcomes were the time to intubation (TTI) and the success rate of ETI. The P value for statistical significance was set at 0.05 and 0.017 in post-hoc test.The success rate of ETI was always 100% regardless of the type of laryngoscope or the bed height. TTI was not significantly different between the 2 bed heights regardless of the type of laryngoscope (all P > 0.05). The time for AWS was the shortest among the 3 laryngoscopes at both bed heights (13.7 ± 3.6 at the minimum bed height and 13.4 ± 4.7 at the maximum bed height) (all P < 0.017). The TTI of Glidescope video laryngoscope was not significantly shorter than that of Macintosh laryngoscope at the minimum height (17.6 ± 4.0 vs 19.6 ± 4.8; P = 0.02).The bed height, whether adjusted to the minimum or maximum setting, did not affect intubation performance. In addition, regardless of the bed height, the intubation time with the video laryngoscopes, especially AWS, was significantly shorter than that with the direct laryngoscope during chest compression.
我们旨在研究在心肺复苏情况下床的高度是否会影响气管插管操作,以及在每个床高条件下哪种喉镜表现最佳。进行了一项随机交叉人体模型研究。招募了21名参与者,并将他们随机分为两组:A组(n = 10)和B组(n = 11)。参与者在进行胸外按压时,以随机顺序使用气道镜(AWS)、Glidescope视频喉镜和Macintosh喉镜进行紧急气管插管(ETI)。每次ETI在两个床高(最低床高:68.9厘米,最高床高:101.3厘米)水平进行。主要结局指标是气管插管时间(TTI)和ETI成功率。事后检验中统计学显著性的P值设定为0.05和0.017。无论喉镜类型或床高如何,ETI成功率始终为100%。无论喉镜类型如何,两个床高之间的TTI均无显著差异(所有P>0.05)。在两个床高条件下,AWS的时间在三种喉镜中都是最短的(最低床高时为13.7±3.6,最高床高时为13.4±4.7)(所有P<0.017)。在最低高度时,Glidescope视频喉镜的TTI不比Macintosh喉镜显著短(17.6±4.0对19.6±4.8;P = 0.02)。床高无论是调整到最低还是最高设置,均不影响插管操作。此外,无论床高如何,在胸外按压期间,视频喉镜尤其是AWS的插管时间明显短于直接喉镜。