Akturk Hacer, Sutcu Murat, Somer Ayper, Aydın Derya, Cihan Rukiye, Ozdemir Aslı, Coban Asuman, Ince Zeynep, Citak Agop, Salman Nuran
Department of Pediatric Infectious Diseases, Istanbul Medical Faculty, Istanbul University, Istanbul, Turkey.
Department of Pediatric Infectious Diseases, Istanbul Medical Faculty, Istanbul University, Istanbul, Turkey.
Braz J Infect Dis. 2016 Mar-Apr;20(2):134-40. doi: 10.1016/j.bjid.2015.12.004. Epub 2016 Feb 8.
Little is known about factors associated with carbapenem-resistant Klebsiella pneumoniae infections in pediatric patients, who are initally colonized with carbapenem-resistant Klebsiella pneumoniae.
A retrospective case-control study was conducted involving pediatric and neonatal intensive care units throughout a five-year period (January 2010-December 2014). Clinical and microbiological data were extracted from Hospital Infection Control Committee reports and patients' medical records. Risk factors were assessed in carbapenem-resistant Klebsiella pneumoniae colonized patients who developed subsequent systemic infection (cases) and compared to carbapenem-resistant Klebsiella pneumoniae colonized patients who did not develop infection (controls).
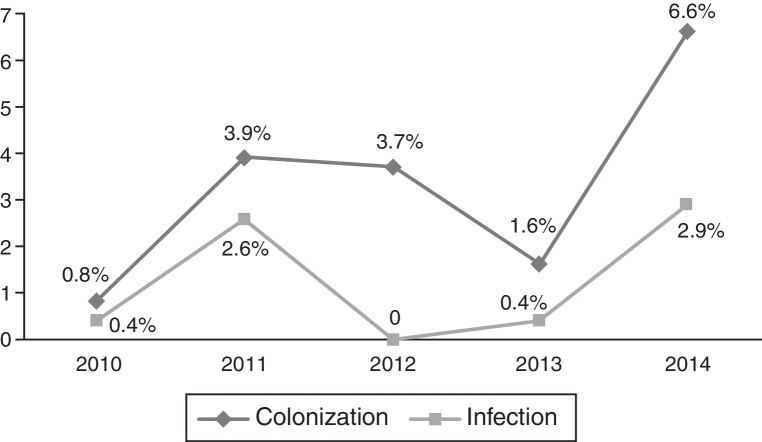
Throughout the study period, 2.6% of patients admitted to neonatal intensive care units and 3.6% of patients admitted to pediatric intensive care units had become colonized with carbapenem-resistant Klebsiella pneumoniae. After a mean of 10.6±1.9 days (median: 7 days, range: 2-38 days) following detection of colonization, 39.0% of the carbapenem-resistant Klebsiella pneumoniae colonized patients in pediatric intensive care units and 18.1% of carbapenem-resistant Klebsiella pneumoniae colonized patients in neonatal intensive care units developed systemic carbapenem-resistant Klebsiella pneumoniae infection. Types of systemic carbapenem-resistant Klebsiella pneumoniae infections included bacteremia (n=15, 62.5%), ventilator-associated pneumonia (n=4, 16.6%), ventriculitis (n=2, 8.3%), intraabdominal infections (n=2, 8.3%), and urinary tract infection (n=1, 4.1%). A logistic regression model including parameters found significant in univariate analysis of carbapenem resistant Klebsiella pneumoniae colonization and carbapenem resistant Klebsiella pneumoniae infection groups revealed underlying metabolic disease (OR: 10.1; 95% CI: 2.7-37.2), previous carbapenem use (OR: 10.1; 95% CI: 2.2-40.1), neutropenia (OR: 13.8; 95% CI: 3.1-61.0) and previous surgical procedure (OR: 7.4; 95% CI: 1.9-28.5) as independent risk factors for carbapenem-resistant Klebsiella pneumoniae infection in patients colonized with carbapenem-resistant Klebsiella pneumoniae. Out of 24 patients with carbapenem resistant Klebsiella pneumoniae infection, 4 (16.6%) died of carbapenem-resistant Klebsiella pneumoniae sepsis.
Asymptomatic colonization with carbapenem-resistant Klebsiella pneumoniae in intensive care units of pediatric departments should alert health care providers about forthcoming carbapenem-resistant Klebsiella pneumoniae infection. Those carbapenem-resistant Klebsiella pneumoniae colonized patients at risk of developing infection due to carbapenem-resistant Klebsiella pneumoniae may be targeted for interventions to reduce subsequent infection occurence and also for timely initiation of empirical carbapenem-resistant Klebsiella pneumoniae active treatment, when necessary.
对于最初定植耐碳青霉烯类肺炎克雷伯菌的儿科患者,与耐碳青霉烯类肺炎克雷伯菌感染相关的因素知之甚少。
进行了一项回顾性病例对照研究,涉及整个五年期间(2010年1月至2014年12月)的儿科和新生儿重症监护病房。临床和微生物学数据从医院感染控制委员会报告和患者病历中提取。对发生后续全身感染的耐碳青霉烯类肺炎克雷伯菌定植患者(病例)的危险因素进行评估,并与未发生感染的耐碳青霉烯类肺炎克雷伯菌定植患者(对照)进行比较。
在整个研究期间,新生儿重症监护病房2.6%的入院患者和儿科重症监护病房3.6%的入院患者定植了耐碳青霉烯类肺炎克雷伯菌。在检测到定植后平均10.6±1.9天(中位数:7天,范围:2 - 38天),儿科重症监护病房39.0%的耐碳青霉烯类肺炎克雷伯菌定植患者和新生儿重症监护病房18.1%的耐碳青霉烯类肺炎克雷伯菌定植患者发生了耐碳青霉烯类肺炎克雷伯菌全身感染。耐碳青霉烯类肺炎克雷伯菌全身感染类型包括菌血症(n = 15,62.5%)、呼吸机相关性肺炎(n = 4,16.6%)、脑室炎(n = 2,8.3%)、腹腔内感染(n = 2,8.3%)和尿路感染(n = 1,4.1%)。一个逻辑回归模型纳入了在耐碳青霉烯类肺炎克雷伯菌定植和耐碳青霉烯类肺炎克雷伯菌感染组单因素分析中发现有意义的参数,结果显示潜在代谢疾病(比值比:10.1;95%置信区间:2.7 - 37.2)、先前使用碳青霉烯类药物(比值比:10.1;95%置信区间:2.2 - 40.1)、中性粒细胞减少(比值比:13.8;95%置信区间:3.1 - 61.0)和先前的外科手术(比值比:7.4;95%置信区间:1.9 - 28.5)是耐碳青霉烯类肺炎克雷伯菌定植患者发生耐碳青霉烯类肺炎克雷伯菌感染的独立危险因素。在24例耐碳青霉烯类肺炎克雷伯菌感染患者中,4例(16.6%)死于耐碳青霉烯类肺炎克雷伯菌败血症。
儿科重症监护病房中耐碳青霉烯类肺炎克雷伯菌的无症状定植应提醒医护人员注意即将发生的耐碳青霉烯类肺炎克雷伯菌感染。那些因耐碳青霉烯类肺炎克雷伯菌而有发生感染风险的耐碳青霉烯类肺炎克雷伯菌定植患者可能是干预的目标,以减少后续感染的发生,并且在必要时及时启动经验性的耐碳青霉烯类肺炎克雷伯菌活性治疗。