Heyderman Robert S, Madhi Shabir A, French Neil, Cutland Clare, Ngwira Bagrey, Kayambo Doris, Mboizi Robert, Koen Anthonet, Jose Lisa, Olugbosi Morounfolu, Wittke Frederik, Slobod Karen, Dull Peter M
Malawi Liverpool Wellcome Trust Clinical Research Programme, University of Malawi College of Medicine, Blantyre, Malawi; Division of Infection and Immunity, University College London, London, UK.
Medical Research Council: Respiratory and Meningeal Pathogens Research Unit, University of the Witwatersrand, Johannesburg, South Africa; Department of Science and Technology/National Research Foundation: Vaccine Preventable Diseases, University of the Witwatersrand, Johannesburg, South Africa; National Institute for Communicable Diseases: a division of National Health Laboratory Service, Centre for Vaccines and Immunology, Johannesburg, South Africa.
Lancet Infect Dis. 2016 May;16(5):546-555. doi: 10.1016/S1473-3099(15)00484-3. Epub 2016 Feb 8.
Neonates born to women infected with HIV are at increased risk for invasive group B streptococcus (GBS) disease. We aimed to compare safety and immunogenicity of trivalent glycoconjugate GBS vaccine in pregnant women with and without HIV in Malawi and South Africa.
In our non-randomised phase 2, open-label, multicentre study, we recruited pregnant women attending two antenatal clinics, one in Blantyre, Malawi, and one in Soweto, Johannesburg, South Africa. Participants were divided into three groups on the basis of their HIV infection status (no infection, infection and high CD4 cell count [>350 cells per μL], and infection and low CD4 cell count [>50 to ≤350 cells per μL]) and received a 5 μg dose of glycoconjugate GBS vaccine (serotypes Ia, Ib, and III, with CRM197 [Novartis Vaccines, Siena, Italy]) intramuscularly at 24-35 weeks' gestation. GBS serotype-specific antibody concentrations were measured before vaccination (day 1), day 15, day 31, and at delivery, and in infants at birth and day 42 of life. The primary outcomes were safety in mothers and infants and the amount of placental transfer of GBS serotype-specific antibodies from mothers to their infants. All immunogenicity and safety analyses were done on the full analysis set, including participants who, or whose mother, correctly received the vaccine and who provided at least one valid assessable serum sample. This study is registered with ClinicalTrials.gov, number NCT01412801.
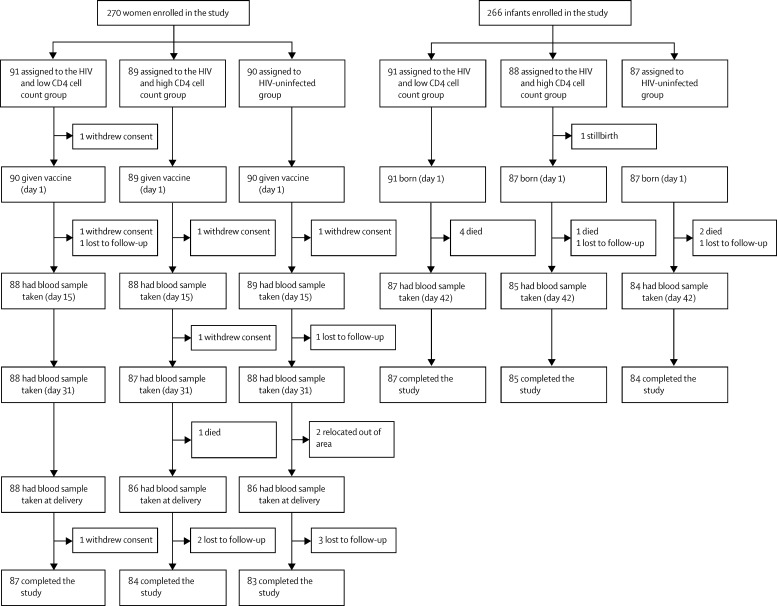
270 women and 266 infants were enrolled between Sept 26, 2011, and Dec 4, 2012 (90 women and 87 infants without HIV, 89 and 88 with HIV and high CD4 cell counts, and 91 and 91 with HIV and low CD4 cell counts, respectively). Seven women were lost to follow-up, six withdrew consent, one died, and two relocated. Eight infants died or were stillborn and two were lost to follow-up. Across serotypes, fold change in antibody concentrations were higher for the HIV-uninfected group than the HIV-infected groups. Transfer ratios were similar across all three groups (0·49-0·72; transfer ratio is infant geometric mean antibody concentration in blood collected within 72 h of birth divided by maternal geometric mean antibody concentration in blood collected at delivery); however, at birth, maternally derived serotype-specific antibody concentrations were lower for infants born to women infected with HIV (0·52-1·62 μg/mL) than for those born to women not infected with HIV (2·67-3·91 μg/mL). 151 (57%) of 265 women reported at least one solicited adverse reaction: 39 (45%) of 87 women with HIV and low CD4 cell counts, 52 (59%) of 88 women with HIV and high CD4 cell counts, and 60 (67%) of 90 women in the HIV-uninfected group. 49 (18%) of 269 women had at least one adverse event deemed possibly related to the vaccine (six [7%] in the HIV and low CD4 cell count group, 12 [13%] in the HIV and high CD4 cell count group, and 21 [23%] in the HIV-uninfected group), as did three (1%) of 266 neonates (zero, two [1%], and one [1%]); none of these events was regarded as serious.
The vaccine was less immunogenic in women infected with HIV than it was in those not infected, irrespective of CD4 cell count, resulting in lower levels of serotype-specific maternal antibody transferred to infants, which could reduce vaccine protection against invasive GBS disease. A validated assay and correlate of protection is needed to understand the potential protective value of this vaccine.
Novartis Vaccines and Diagnostics division (now part of the GlaxoSmithKline group of companies), Wellcome Trust UK, Medical Research Council: Respiratory and Meningeal Pathogens Research Unit.
感染HIV的女性所生新生儿患B族链球菌(GBS)侵袭性疾病的风险增加。我们旨在比较三价糖共轭GBS疫苗在马拉维和南非感染HIV和未感染HIV的孕妇中的安全性和免疫原性。
在我们的非随机2期开放标签多中心研究中,我们招募了在两家产前诊所就诊的孕妇,一家在马拉维的布兰太尔,另一家在南非约翰内斯堡的索韦托。参与者根据其HIV感染状况分为三组(未感染、感染且CD4细胞计数高[>350个/μL]、感染且CD4细胞计数低[>50至≤350个/μL]),并在妊娠24 - 35周时肌肉注射5μg剂量的糖共轭GBS疫苗(血清型Ia、Ib和III,与CRM197[诺华疫苗公司,意大利锡耶纳])。在接种疫苗前(第1天)、第15天、第31天、分娩时以及婴儿出生时和出生后第42天测量GBS血清型特异性抗体浓度。主要结局是母亲和婴儿的安全性以及GBS血清型特异性抗体从母亲到婴儿的胎盘转移量。所有免疫原性和安全性分析均在完整分析集上进行,包括正确接种疫苗且提供至少一份有效可评估血清样本的参与者本人或其母亲。本研究已在ClinicalTrials.gov注册,注册号为NCT01412801。
2011年9月26日至2012年12月4日期间共纳入270名女性和266名婴儿(分别为90名未感染HIV的女性和87名婴儿、89名感染HIV且CD4细胞计数高的女性和88名婴儿、91名感染HIV且CD4细胞计数低的女性和91名婴儿)。7名女性失访,6名撤回同意书,1名死亡,2名搬迁。8名婴儿死亡或死产,2名失访。在所有血清型中,未感染HIV组的抗体浓度变化倍数高于感染HIV组。三组的转移率相似(0.49 - 0.72;转移率是出生后72小时内采集的婴儿血液中几何平均抗体浓度除以分娩时采集的母亲血液中几何平均抗体浓度);然而,出生时,感染HIV的女性所生婴儿的母源血清型特异性抗体浓度(0.52 - 1.62μg/mL)低于未感染HIV的女性所生婴儿(2.67 - 3.91μg/mL)。265名女性中有151名(57%)报告了至少一种预期不良反应:87名感染HIV且CD4细胞计数低的女性中有39名(45%)、88名感染HIV且CD4细胞计数高的女性中有52名(59%)、90名未感染HIV的女性中有60名(67%)。269名女性中有49名(18%)发生了至少一种被认为可能与疫苗相关的不良事件(感染HIV且CD4细胞计数低的组中有6名[7%]、感染HIV且CD4细胞计数高的组中有12名[13%]、未感染HIV的组中有21名[23%]),266名新生儿中有3名(1%)发生了此类事件(分别为0名、2名[1%]和1名[1%]);这些事件均不被视为严重事件。
无论CD4细胞计数如何,该疫苗在感染HIV的女性中的免疫原性均低于未感染HIV的女性,导致转移至婴儿的血清型特异性母源抗体水平较低,这可能会降低疫苗对GBS侵袭性疾病的保护作用。需要一种经过验证的检测方法和保护相关性来了解该疫苗的潜在保护价值。
诺华疫苗和诊断部门(现为葛兰素史克公司集团的一部分)、英国惠康信托基金会、医学研究理事会:呼吸和脑膜病原体研究组。