Axelrod D A, Naik A S, Schnitzler M A, Segev D L, Dharnidharka V R, Brennan D C, Bae S, Chen J, Massie A, Lentine K L
Section of Solid Organ Transplantation, Department of Surgery, Dartmouth Hitchcock Medical Center, Lebanon, NH.
Division of Nephrology, Department of Internal Medicine, University of Michigan, Ann Arbor, MI.
Am J Transplant. 2016 Aug;16(8):2453-62. doi: 10.1111/ajt.13758. Epub 2016 Mar 31.
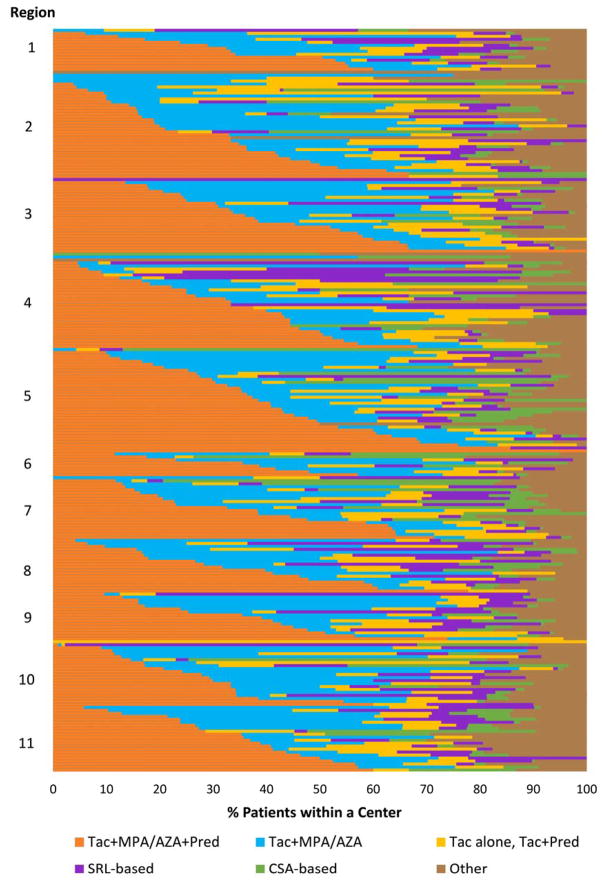
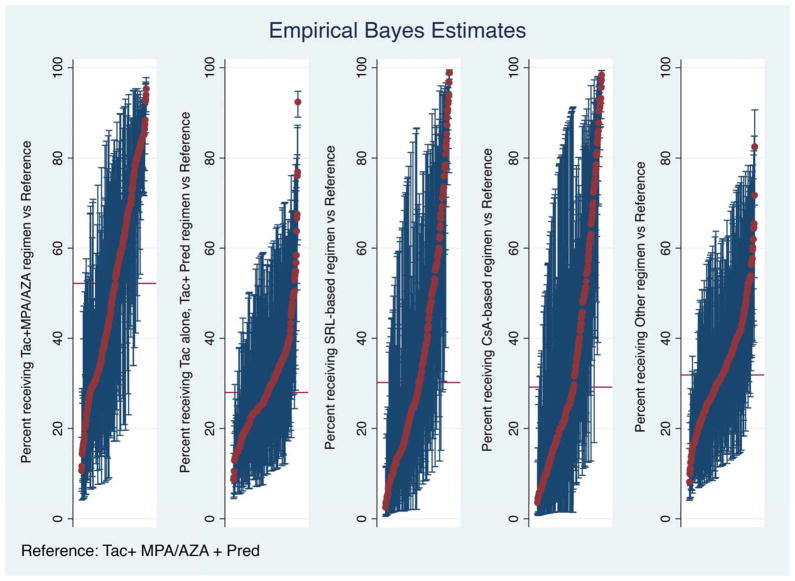
Immunosuppression management in kidney transplantation has evolved to include an increasingly diverse choice of medications. Although informed by patient and donor characteristics, choice of immunosuppression regimen varies widely across transplant programs. Using a novel database integrating national transplant registry and pharmacy fill records, immunosuppression use at 6-12 and 12-24 mo after transplant was evaluated for 22 453 patients transplanted in 249 U.S. programs in 2005-2010. Use of triple immunosuppression comprising tacrolimus, mycophenolic acid or azathioprine, and steroids varied widely (0-100% of patients per program), as did use of steroid-sparing regimens (0-77%), sirolimus-based regimens (0-100%) and cyclosporine-based regimens (0-78%). Use of triple therapy was more common in highly sensitized patients, women and recipients with dialysis duration >5 years. Sirolimus use appeared to diminish over the study period. Patient and donor characteristics explained only a limited amount of the observed variation in regimen use, whereas center choice explained 30-46% of the use of non-triple-therapy immunosuppression. The majority of patients who received triple-therapy (79%), cyclosporine-based (87.6%) and sirolimus-based (84.3%) regimens continued them in the second year after transplant. This population-based study of immunosuppression practice demonstrates substantial variation in center practice beyond that explained by differences in patient and donor characteristics.
肾移植中的免疫抑制管理已经发展到包括越来越多样化的药物选择。尽管免疫抑制方案的选择受患者和供体特征的影响,但不同移植项目之间的差异很大。利用一个整合了国家移植登记处和药房配药记录的新型数据库,对2005年至2010年在美国249个项目中接受移植的22453名患者在移植后6至12个月和12至24个月的免疫抑制药物使用情况进行了评估。包含他克莫司、霉酚酸或硫唑嘌呤以及类固醇的三联免疫抑制的使用差异很大(每个项目中使用该方案的患者比例为0至100%),无类固醇方案(0至77%)、西罗莫司方案(0至100%)和环孢素方案(0至78%)的使用情况也是如此。三联疗法在高敏患者、女性以及透析时间>5年的受者中更为常见。在研究期间,西罗莫司的使用似乎有所减少。患者和供体特征仅解释了观察到的方案使用差异中的有限部分,而中心选择解释了30%至46%的非三联疗法免疫抑制的使用情况。接受三联疗法(79%)、环孢素方案(87.6%)和西罗莫司方案(84.3%)的大多数患者在移植后的第二年仍继续使用这些方案。这项基于人群的免疫抑制实践研究表明,除了患者和供体特征差异所解释的部分外,中心实践存在很大差异。