Sømod Mia Elbek, Vestergaard Esben Thyssen, Kristensen Kurt, Birkebæk Niels Holtum
Department of Pediatrics, Aarhus University Hospital, Skejby, Palle Juul Jensens Boulevard 99, DK-8200 Aarhus N, Denmark.
Medical Research Laboratory, Aarhus University, Nørrebrogade 44 building 3B, DK-8000 Aarhus C, Denmark.
Int J Pediatr Endocrinol. 2016;2016:4. doi: 10.1186/s13633-016-0022-x. Epub 2016 Feb 22.
Premature thelarche (PT) seems to be increasing and it is difficult to differentiate its early stages from precocious puberty (PP). Clinical and biochemical parameters are warranted to differentiate the two diagnoses.
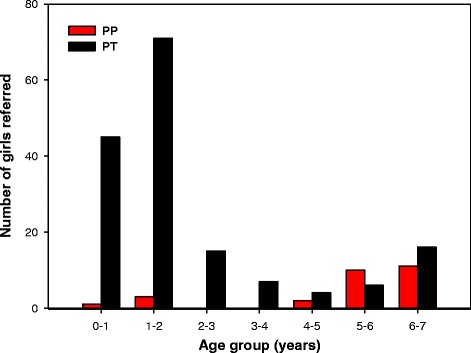
One hundred ninety-one girls aged 0.5-7 years were included. Diagnoses were validated and the girls were categorized to the groups PP (n = 27) and PT (n = 164). Anthropometry, Tanner stages, ethnicity, bone age, and biochemistry, were recorded. Conventional variables for diagnosing PP were compared between the groups at time of referral to identify parameters predictive for the diagnosis.
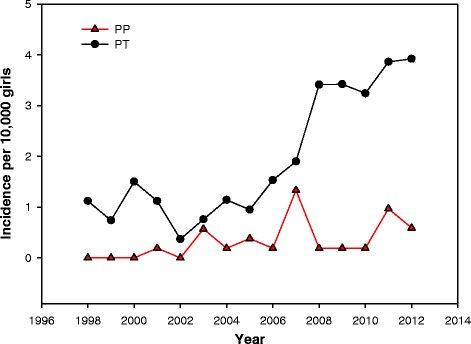
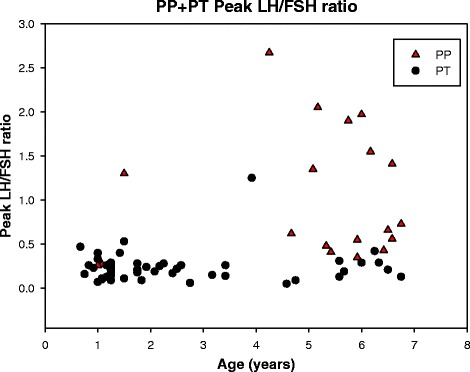
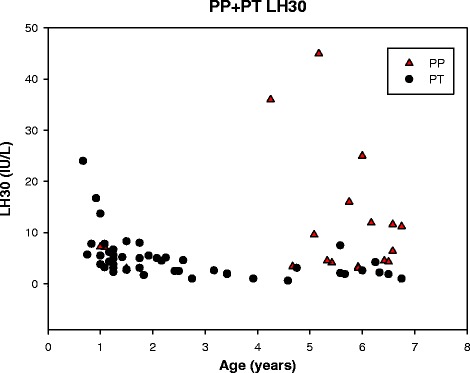
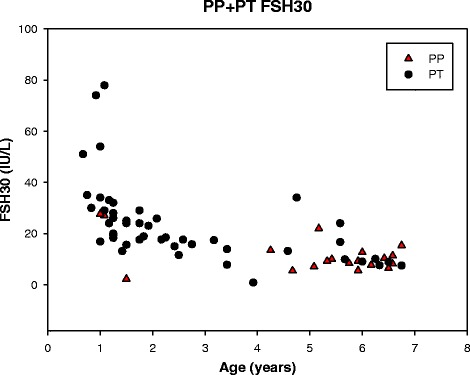
The referral rate of PT increased from 1998-2013. Girls with PT and PP differed with regards to age at referral, body mass index standard deviation scores (BMISDS), ethnicity, bone age advancement, basal luteinizing hormone (LH), gonadotropin releasing hormone (GnRH) stimulated LH and follicle stimulating hormone (FSH), basal and stimulated LH/FSH ratio, and sex-hormone binding globulin (SHBG). Apart from SHBG there was considerable overlap of the variables between the PT and the PP groups.
First, the incidence of PT appears to increase. Second, SHBG was the variable which best discriminated PT from PP. Third, stimulated LH in 1-3 years old girls with PT is similar to stimulated LH in 5-7 years old girls with PP. Age, BMISDS, ethnicity, bone age, stimulated gonadotropins and LH/FSH and SHBG are all useful variables for differentiating PP from PT. However normative data for stimulated LH and FSH in the age group 0.5-7 years are warranted.
早熟乳房发育(PT)的发病率似乎在上升,且很难将其早期阶段与性早熟(PP)区分开来。需要临床和生化参数来鉴别这两种诊断。
纳入191名年龄在0.5至7岁的女孩。对诊断进行验证,并将女孩分为性早熟组(n = 27)和早熟乳房发育组(n = 164)。记录人体测量学指标、坦纳分期、种族、骨龄和生化指标。比较转诊时两组间诊断性早熟的传统变量,以确定预测诊断的参数。
1998年至2013年期间,早熟乳房发育的转诊率有所上升。早熟乳房发育组和性早熟组女孩在转诊年龄、体重指数标准差评分(BMISDS)、种族、骨龄进展、基础促黄体生成素(LH)、促性腺激素释放激素(GnRH)刺激后的LH和促卵泡生成素(FSH)、基础及刺激后的LH/FSH比值以及性激素结合球蛋白(SHBG)方面存在差异。除SHBG外,早熟乳房发育组和性早熟组之间的变量有相当大的重叠。
第一,早熟乳房发育的发病率似乎在增加。第二,SHBG是最能区分早熟乳房发育和性早熟的变量。第三,1至3岁早熟乳房发育女孩刺激后的LH与5至7岁性早熟女孩刺激后的LH相似。年龄、BMISDS、种族、骨龄、刺激后的促性腺激素、LH/FSH和SHBG都是区分性早熟和早熟乳房发育的有用变量。然而,0.5至7岁年龄组刺激后的LH和FSH的规范数据是必要的。