Chakravarty Tarun, Sharma Rahul, Abramowitz Yigal, Kapadia Samir, Latib Azeem, Jilaihawi Hasan, Poddar Kanhaiya Lal, Giustino Gennaro, Ribeiro Henrique B, Tchetche Didier, Monteil Benoit, Testa Luca, Tarantini Giuseppe, Facchin Michela, Lefèvre Thierry, Lindman Brian R, Hariri Babak, Patel Jigar, Takahashi Nobuyuki, Matar George, Mirocha James, Cheng Wen, Tuzcu Murat E, Sievert Horst, Rodés-Cabau Josep, Colombo Antonio, Finkelstein Ariel, Fajadet Jean, Makkar Raj R
Cedars-Sinai Heart Institute, Los Angeles, California.
Cedars-Sinai Heart Institute, Los Angeles, California; Tel Aviv Medical Center, Tel Aviv, Israel.
J Am Coll Cardiol. 2016 Mar 1;67(8):951-960. doi: 10.1016/j.jacc.2015.10.103.
A percutaneous approach with transcatheter aortic valve replacement (TAVR) and percutaneous coronary intervention (PCI) of the left main coronary artery (LM) is frequently used in high-risk patients with coexisting aortic stenosis and LM disease. Outcomes of TAVR plus LM PCI have not been previously reported.
The primary objective of the TAVR-LM registry is to evaluate clinical outcomes in patients undergoing TAVR plus LM PCI.
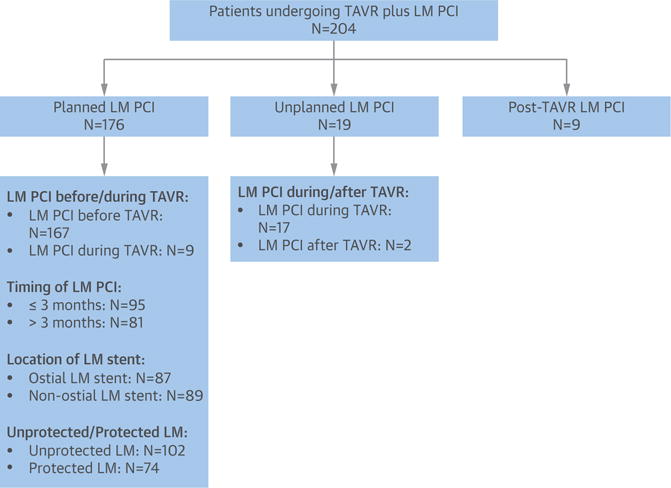
Clinical, echocardiographic, computed tomographic, and angiographic characteristics were retrospectively collected in 204 patients undergoing TAVR plus LM PCI. In total, 128 matched patient pairs were generated by performing 1:1 case-control matching between 167 patients with pre-existing LM stents undergoing TAVR and 1,188 control patients undergoing TAVR without LM revascularization.
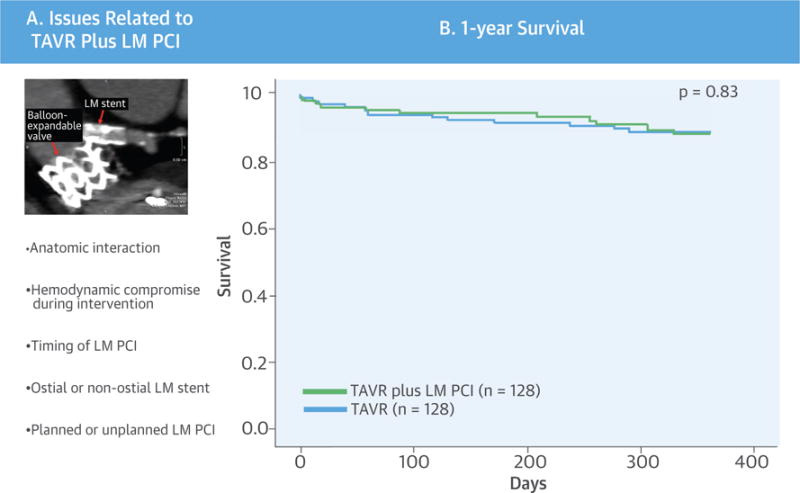
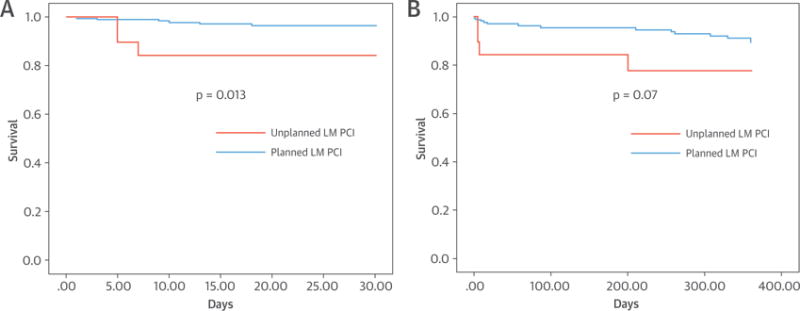
One-year mortality (9.4% vs. 10.2%, p = 0.83) was similar between the TAVR plus LM PCI cohort and matched controls. One-year mortality after TAVR plus LM PCI was not different in patients with unprotected compared with protected LMs (7.8% vs. 8.1%, p = 0.88), those undergoing LM PCI within 3 months compared with those with LM PCI greater than 3 months before TAVR (7.4% vs. 8.6%, p = 0.61), and those with ostial versus nonostial LM stents (10.3% vs. 15.6%, p = 0.20). Unplanned LM PCI performed because of TAVR-related coronary complication, compared with planned LM PCI performed for pre-existing LM disease, resulted in increased 30-day (15.8% vs. 3.4%, p = 0.013) and 1-year (21.1% vs. 8.0%, p = 0.071) mortality.
Despite the anatomic proximity of the aortic annulus to the LM, TAVR plus LM PCI is safe and technically feasible, with short- and intermediate-term clinical outcomes comparable with those in patients undergoing TAVR alone. These results suggest that TAVR plus LM PCI is a reasonable option for patients who are at high risk for surgery.
经皮主动脉瓣置换术(TAVR)联合经皮左主干冠状动脉(LM)介入治疗(PCI)的经皮入路常用于合并主动脉瓣狭窄和LM病变的高危患者。此前尚未报道过TAVR联合LM PCI的治疗结果。
TAVR-LM注册研究的主要目的是评估接受TAVR联合LM PCI患者的临床结局。
回顾性收集204例接受TAVR联合LM PCI患者的临床、超声心动图、计算机断层扫描和血管造影特征。通过对167例既往有LM支架置入且接受TAVR的患者与1188例未进行LM血运重建且接受TAVR的对照患者进行1:1病例对照匹配,共生成128对匹配患者。
TAVR联合LM PCI队列与匹配对照组的1年死亡率相似(9.4%对10.2%,p = 0.83)。未保护LM患者与保护LM患者在TAVR联合LM PCI后的1年死亡率无差异(7.8%对8.1%,p = 0.88),TAVR前3个月内接受LM PCI的患者与TAVR前3个月以上接受LM PCI的患者的1年死亡率无差异(7.4%对8.6%,p = 0.61),开口处LM支架患者与非开口处LM支架患者的1年死亡率无差异(10.3%对15.6%,p = 0.20)。因TAVR相关冠状动脉并发症而进行的非计划性LM PCI与因既往LM病变而进行的计划性LM PCI相比,导致30天(15.8%对3.4%,p = 0.013)和1年(21.1%对8.0%,p = 0.071)死亡率增加。
尽管主动脉瓣环与LM在解剖位置上接近,但TAVR联合LM PCI是安全且技术上可行的,其短期和中期临床结局与单纯接受TAVR的患者相当。这些结果表明,TAVR联合LM PCI对于手术高危患者是一个合理的选择。