Xu Ning, Chen Juan, Chang Xin, Zhang Jingwen, Liu Qinghua, Li Aljun, Lin Dianjie
Dr. Dianjie Lin, No. 9677, The Olympic Mid Road,, Lixia District jinan Shandong, 250100 China, T: +86-0531-68773269,
Ann Saudi Med. 2016 Jan-Feb;36(1):37-41. doi: 10.5144/0256-4947.2016.37.
Chronic obstructive pulmonary disease (COPD) is one of the leading causes of mortality and morbidity worldwide. However, there are still no easily obtained biomarkers for prognosis. As a high-affinity Fc receptor, CD64 is an early marker of immune response to bacterial infection, but its role in acute exacerbation of COPD (AECOPD) remains incompletely understood.
We investigated the prognostic role of the neutrophial CD64 (nCD64) index in AECOPD patients.
Retrospective cross-sectional study of all patient admitted between January 2013 to May 2014.
Provincial hospitals affiliated with a university.
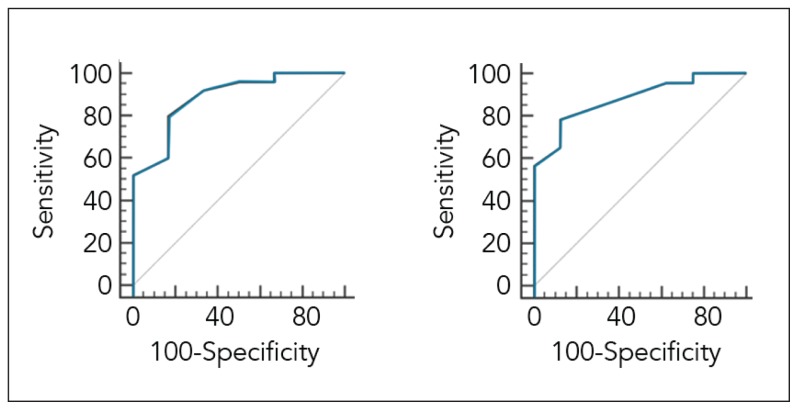
Clinical and laboratory data were collected in patients admitted for AECOPD and stable COPD patients, in whom nCD64 index was obtained. A receiver operating characteristics curve was used to determine the optimal cut-off levels for the nCD64 index that discriminated survivors versus nonsurvivors during index hospitalization, and during a post-discharge period of 12 months.
nCD64 index level.
The white blood cell count, CRP (C-reactive protein (CRP) and PCT (procalcitonin) in AECOPD subjects (n=31) were all significantly higher than in controls (n=18) (P= 3.3 predicted in-hospital mortality with a sensitivity and specificity of 80% and 83%, respectively (area under the ROC=0.887; 95% confidence interval [CI]=0.721-0.972, P < .001). An nCD64 index of 3.3 upon admission as the optimal cut-off level to predict post-discharge mortality had a sensitivity and specificity of 83% and 75%, respectively (area under the ROC=0.842; 95% confidence interval [CI]=0.667-0.948, P < .001).
An elevated nCD64 index was a reliable prognostic biomarker for both short-term and long-term mortality in patients admitted for AECOPD.
Retrospective design prevented collection of enough evidence to demonstrate infectious origin for COPD in every patient. Unsure whether nCD64 differed between bacterial and viral exacerbation.
慢性阻塞性肺疾病(COPD)是全球死亡和发病的主要原因之一。然而,目前仍没有易于获得的用于预后评估的生物标志物。作为一种高亲和力Fc受体,CD64是细菌感染免疫反应的早期标志物,但其在慢性阻塞性肺疾病急性加重(AECOPD)中的作用仍不完全清楚。
我们研究了中性粒细胞CD64(nCD64)指数在AECOPD患者中的预后作用。
对2013年1月至2014年5月期间收治的所有患者进行回顾性横断面研究。
某大学附属医院。
收集因AECOPD入院患者和稳定期COPD患者的临床和实验室数据,并检测nCD64指数。采用受试者工作特征曲线确定nCD64指数在本次住院期间及出院后12个月区分存活者与非存活者的最佳临界值。
nCD64指数水平。
AECOPD患者(n = 31)的白细胞计数、C反应蛋白(CRP)和降钙素原(PCT)均显著高于对照组(n = 18)(P < 0.001)。nCD64指数≥3.3预测住院死亡率为3.3%,敏感性和特异性分别为80%和83%(ROC曲线下面积=0.887;95%置信区间[CI]=0.721 - 0.972,P < 0.001)。以入院时nCD64指数≥3.3作为预测出院后死亡率的最佳临界值,敏感性和特异性分别为83%和75%(ROC曲线下面积=0.842;95%置信区间[CI]=0.667 - 0.948,P < 0.001)。
nCD64指数升高是AECOPD入院患者短期和长期死亡率的可靠预后生物标志物。
回顾性设计妨碍收集足够证据以证明每位患者COPD的感染源。不确定细菌和病毒加重时nCD64是否存在差异。