Xu Xiao-Ling, Dan Li, Chen Wei, Zhu Shuang-Mei, Mao Wei-Min
Key Laboratory of Diagnosis and Treatment Technology for Thoracic Cancer, Zhejiang Cancer Research Institute, Zhejiang Province Cancer Hospital, Zhejiang Cancer Center, Hangzhou, People's Republic of China.
Department of Radiotherapy, Lishui People's Hospital, Lishui, People's Republic of China.
Onco Targets Ther. 2016 Feb 22;9:845-53. doi: 10.2147/OTT.S95511. eCollection 2016.
Approximately 30% of all cases of nonsmall-cell lung cancer (NSCLC) are of a locally advanced (IIIA or IIIB) stage. However, surgical therapy for patients with stage IIIA (N2) NSCLC is associated with a disappointing 5-year survival rate. The optimal treatment for stage IIIA (N2) NSCLC is still in dispute.
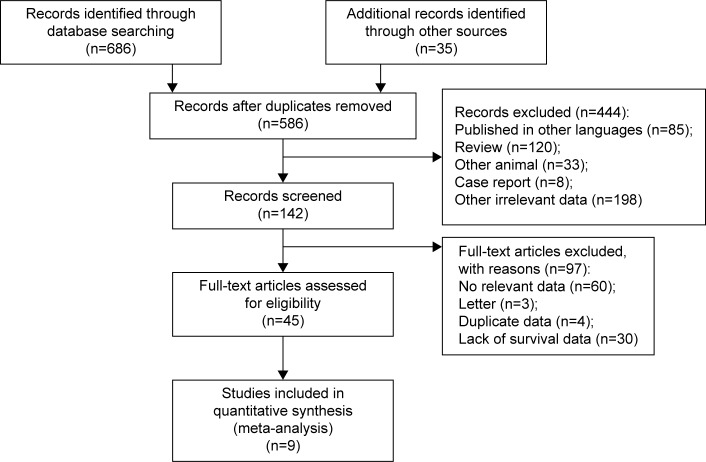
A literature search was performed in the PubMed, Embase, and MEDLINE databases (last search updated in March 2015), and a meta-analysis of the available data was conducted. Two authors independently extracted data from each eligible study.
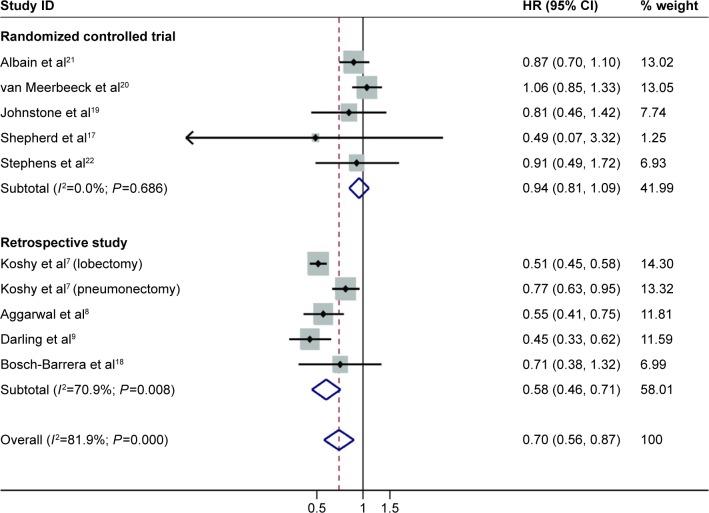
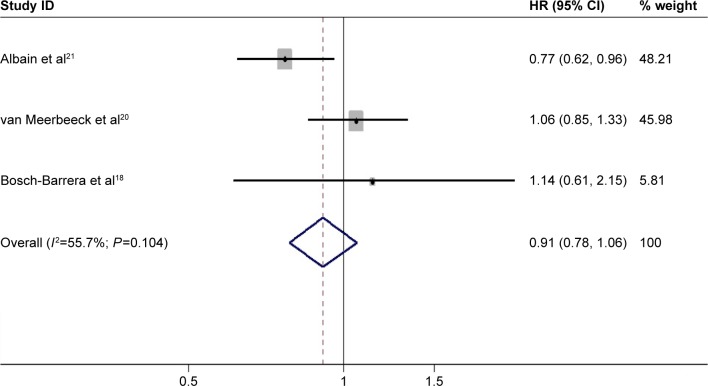
A total of nine studies, including five randomized controlled trials and four retrospective studies, were enrolled in this meta-analysis. Significant homogeneity (χ (2)=49.62, P=0.000, I (2)=81.9%) was detected between four of the studies, including a total of 11,948 selected cases. Among the nine studies that investigated overall survival, the pooled hazard ratio (HR) was 0.70 (95% confidence interval (CI): 0.56-0.87; P=0.000). Subgroup analyses were performed according to the study design and the extent of resection. We observed a statistically significant better outcome after lobectomy (pooled HR: 0.52; 95% CI: 0.47-0.58; P=0.000) than after pneumonectomy (pooled HR: 0.82; 95% CI: 0.69-0.98; P=0.028). Unfortunately, there was no significant difference between the randomized controlled studies, as the pooled HR was 0.94 (95% CI: 0.81-1.09; P=0.440).
Neoadjuvant chemoradiotherapy or chemotherapy followed by surgery (particularly lobectomy) is superior to following these therapies with definitive chemoradiation or radiotherapy, particularly in patients undergoing lobectomy.
在所有非小细胞肺癌(NSCLC)病例中,约30%为局部晚期(IIIA期或IIIB期)。然而,IIIA期(N2)NSCLC患者的手术治疗5年生存率令人失望。IIIA期(N2)NSCLC的最佳治疗方案仍存在争议。
在PubMed、Embase和MEDLINE数据库中进行文献检索(最后一次检索更新于2015年3月),并对现有数据进行荟萃分析。两位作者独立从每项符合条件的研究中提取数据。
本荟萃分析共纳入9项研究,包括5项随机对照试验和4项回顾性研究。在其中4项研究(共11948例入选病例)之间检测到显著的同质性(χ(2)=49.62,P=0.000,I(2)=81.9%)。在9项研究总体生存情况的研究中,合并风险比(HR)为0.70(95%置信区间(CI):0.56 - 0.87;P=0.000)。根据研究设计和切除范围进行亚组分析。我们观察到肺叶切除术后的结果在统计学上显著优于全肺切除术后(合并HR:0.52;95%CI:0.