Chen Weiping, Li Qiken, Fan Yongtian, Li Dechuan, Jiang Lai, Qiu Pengnian, Tang Lilong
Department of Colorectal Surgery, Zhejiang Cancer Hospital, Hangzhou, Zhejiang, 310022, China.
Department of Radiology, Zhejiang Cancer Hospital, Hangzhou, Zhejiang, 310022, China.
PLoS One. 2016 Mar 18;11(3):e0151773. doi: 10.1371/journal.pone.0151773. eCollection 2016.
Laparoscopic sphincter-preserving low anterior resection for rectal cancer is a surgery demanding great skill. Immense efforts have been devoted to identifying factors that can predict operative difficulty, but the results are inconsistent.
Our study was conducted to screen patients' factors to build models for predicting the operative difficulty using well controlled data.
We retrospectively reviewed records of 199 consecutive patients who had rectal cancers 5-8 cm from the anal verge. All underwent laparoscopic sphincter-preserving low anterior resections with total mesorectal excision (TME) and double stapling technique (DST). Data of 155 patients from one surgeon were utilized to build models to predict standardized endpoints (operative time, blood loss) and postoperative morbidity. Data of 44 patients from other surgeons were used to test the predictability of the built models.
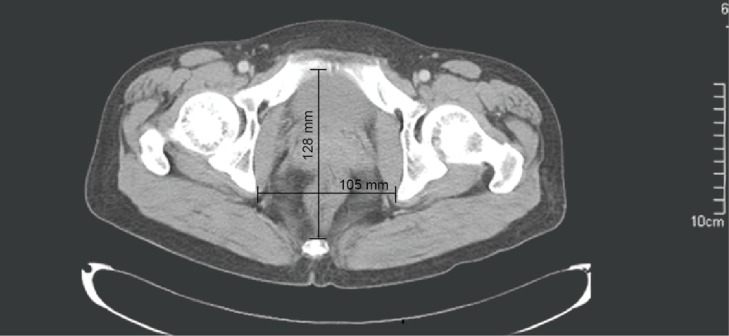
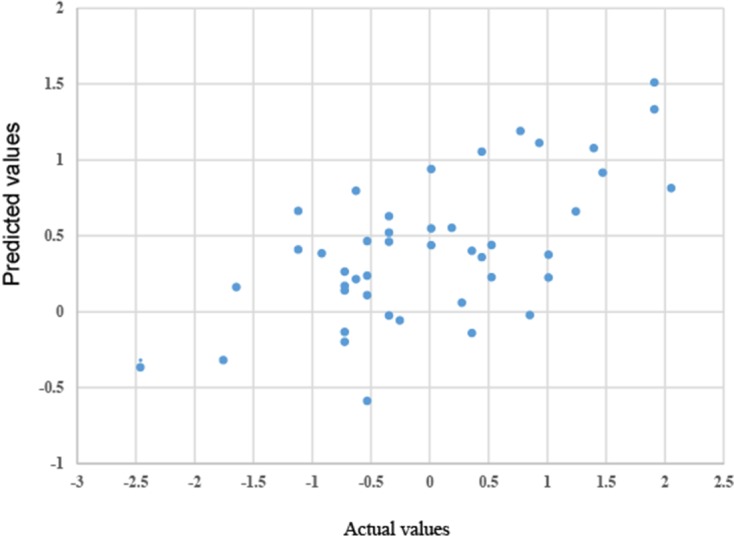
Our results showed prior abdominal surgery, preoperative chemoradiotherapy, tumor distance to anal verge, interspinous distance, and BMI were predictors for the standardized operative times. Gender and tumor maximum diameter were related to the standardized blood loss. Temporary diversion and tumor diameter were predictors for postoperative morbidity. The model constructed for the operative time demonstrated excellent predictability for patients from different surgeons.
With a well-controlled patient population, we have built a predictable model to estimate operative difficulty. The standardized operative time will make it possible to significantly increase sample size and build more reliable models to predict operative difficulty for clinical use.
腹腔镜保留括约肌低位前切除术治疗直肠癌是一项技术要求很高的手术。人们已付出巨大努力来确定可预测手术难度的因素,但结果并不一致。
我们开展本研究以筛选患者因素,利用严格控制的数据建立预测手术难度的模型。
我们回顾性分析了199例距肛缘5 - 8 cm直肠癌患者的记录。所有患者均接受了腹腔镜保留括约肌低位前切除术,并采用了全直肠系膜切除术(TME)和双吻合器技术(DST)。利用一位外科医生的155例患者数据建立模型,以预测标准化终点(手术时间、失血量)和术后发病率。另外44例来自其他外科医生的患者数据用于检验所建模型的预测能力。
我们的结果显示,既往腹部手术、术前放化疗、肿瘤距肛缘距离、棘间距离和体重指数是标准化手术时间的预测因素。性别和肿瘤最大直径与标准化失血量有关。临时造口和肿瘤直径是术后发病率的预测因素。所构建的手术时间模型对不同外科医生的患者显示出优异的预测能力。
在严格控制的患者群体中,我们建立了一个可预测手术难度的模型。标准化手术时间将有可能显著增加样本量,并建立更可靠的模型来预测手术难度以供临床使用。