Centre for Women's Health Research, University of Liverpool and Liverpool Women's Hospital, Liverpool, UK.
School of Social and Community Medicine, University of Bristol, Bristol, UK.
BJOG. 2016 Aug;123(9):1462-70. doi: 10.1111/1471-0528.13981. Epub 2016 Mar 22.
To compare the clinical effectiveness and cost-effectiveness of labour induction methods.
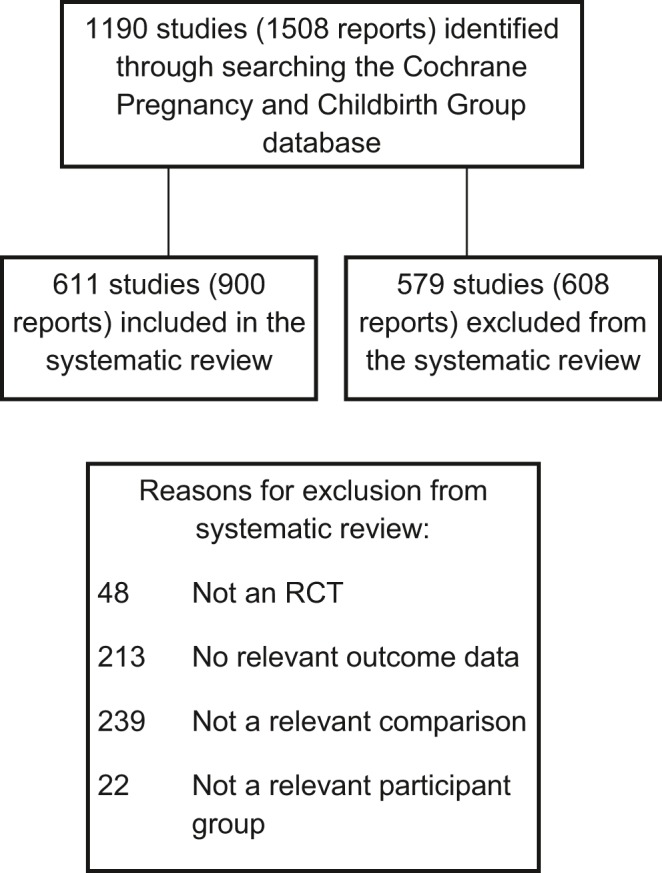
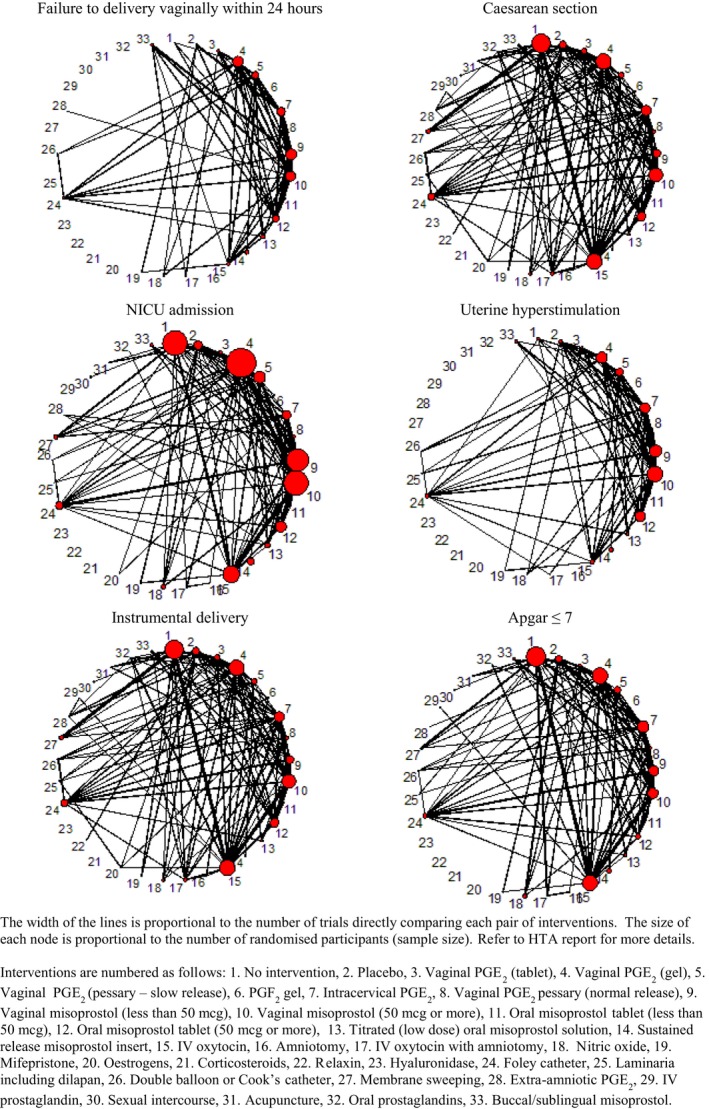
We conducted a systematic review of randomised trials comparing interventions for third-trimester labour induction (search date: March 2014). Network meta-analysis was possible for six of nine prespecified key outcomes: vaginal delivery within 24 hours (VD24), caesarean section, uterine hyperstimulation, neonatal intensive care unit (NICU) admissions, instrumental delivery and infant Apgar scores. We developed a decision-tree model from a UK NHS perspective and calculated incremental cost-effectiveness ratios, expected costs, utilities and net benefit, and cost-effectiveness acceptability curves.
In all, 611 studies comparing 31 active interventions were included. Intravenous oxytocin with amniotomy and vaginal misoprostol (≥50 μg) were most likely to achieve VD24. Titrated low-dose oral misoprostol achieved the lowest odds of caesarean section, but there was considerable uncertainty in ranking estimates. Vaginal (≥50 μg) and buccal/sublingual misoprostol were most likely to increase uterine hyperstimulation with high uncertainty in ranking estimates. Compared with placebo, extra-amniotic prostaglandin E2 reduced NICU admissions. There were insufficient data to conduct analyses for maternal and neonatal mortality and serious morbidity or maternal satisfaction. Conclusions were robust after exclusion of studies at high risk of bias. Due to poor reporting of VD24, the cost-effectiveness analysis compared a subset of 20 interventions. There was considerable uncertainty in estimates, but buccal/sublingual and titrated (low-dose) misoprostol showed the highest probability of being most cost-effective.
Future trials should be designed and powered to detect a method that is more cost-effective than low-dose titrated oral misoprostol.
New study ranks methods to induce labour in pregnant women on effectiveness and cost.
比较分娩诱导方法的临床效果和成本效益。
我们对比较妊娠晚期分娩诱导干预措施的随机试验进行了系统评价(检索日期:2014 年 3 月)。对于九个预先指定的关键结局中的六个,我们进行了网络荟萃分析:24 小时内阴道分娩(VD24)、剖宫产、子宫过度刺激、新生儿重症监护病房(NICU)入院、器械分娩和婴儿 Apgar 评分。我们从英国国民健康保险制度的角度制定了决策树模型,并计算了增量成本效益比、预期成本、效用和净收益,以及成本效益可接受性曲线。
共纳入 611 项比较 31 种干预措施的研究。静脉滴注催产素联合羊膜穿刺术和阴道米索前列醇(≥50μg)最有可能实现 VD24。滴定低剂量口服米索前列醇剖宫产率最低,但排序估计存在很大的不确定性。阴道(≥50μg)和颊/舌下米索前列醇最有可能增加子宫过度刺激,排序估计的不确定性很高。与安慰剂相比,羊膜外前列腺素 E2 可降低 NICU 入院率。由于缺乏关于产妇和新生儿死亡率以及严重发病率或产妇满意度的数据分析,因此无法进行分析。在排除高偏倚风险的研究后,结论仍然可靠。由于 VD24 报告不佳,成本效益分析比较了 20 种干预措施的子集。估计值存在很大的不确定性,但颊/舌下和滴定(低剂量)米索前列醇显示出最高的最具成本效益的可能性。
未来的试验应设计和实施,以检测出一种比低剂量滴定口服米索前列醇更具成本效益的方法。
比较了不同分娩诱导方法的临床效果和成本效益。
网络荟萃分析了 6 个关键结局,包括阴道分娩、剖宫产、子宫过度刺激、新生儿重症监护病房入院、器械分娩和婴儿 Apgar 评分。
从英国国民健康保险制度的角度制定了决策树模型,计算了增量成本效益比、预期成本、效用和净收益,以及成本效益可接受性曲线。
结论表明,低剂量滴定口服米索前列醇是目前最具成本效益的分娩诱导方法,但未来的研究需要设计和实施更具成本效益的方法。