Gofrit Ofer N, Yutkin Vladimir, Shapiro Amos, Pizov Galina, Zorn Kevin C, Hidas Guy, Gielchinsky Ilan, Duvdevani Mordechai, Landau Ezekiel H, Pode Dov
Department of Urology, Hadassah Hebrew University Medical Center , Jerusalem , Israel.
Department of Pathology, Hadassah Hebrew University Medical Center , Jerusalem , Israel.
Front Oncol. 2016 Mar 15;6:43. doi: 10.3389/fonc.2016.00043. eCollection 2016.
High-grade urothelial carcinomas (UCs) often show foci of variant differentiation. There is limited information in the literature about the response of these variant urothelial tumors to immunotherapy with bacillus Calmette-Guerin (BCG). We compared the response, to treatment with BCG, of UC containing glandular, squamous, nested, and micropapillary types of differentiation to response of conventional non-muscle invasive high-grade UC.
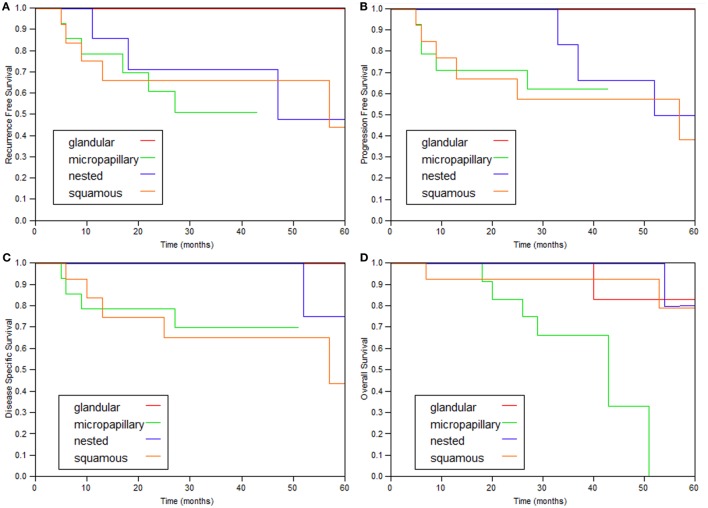
A total of 100 patients were diagnosed with variant histology urothelial cancer between June 1995 and December 2013. Forty-one patients with Ta or T1, confirmed by second look biopsies, received immunotherapy with BCG. Fourteen patients in this group were diagnosed with micropapillary differentiation, 13 patients with squamous differentiation, 9 patients with glandular differentiation, and 7 patients with nested variants. The control group included 140 patients with conventional high-grade UC. Both groups have been treated and followed similarly.
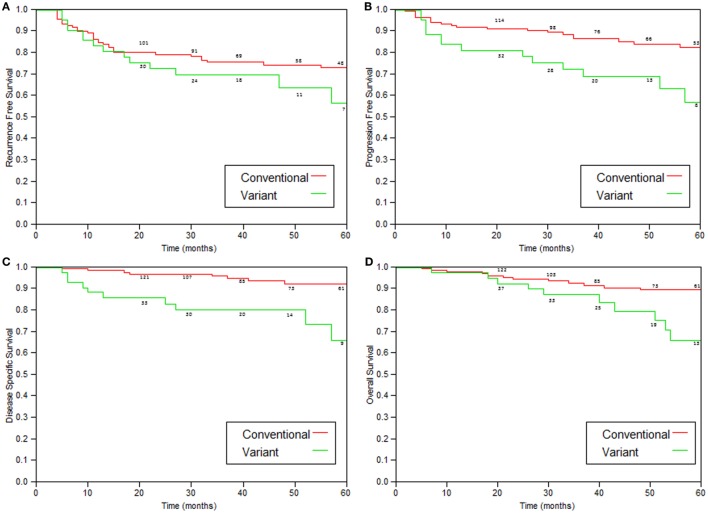
Patients with variant tumors had similar clinical features to patients with conventional disease, including age, male to female ratio, stage, the presence of Tis, and median follow-up. Patients with variant tumors had a significantly worse prognosis compared to patients with conventional high-grade UC, including 5-year recurrence-free survival (63.5 Vs. 71.5%, p = 0.05), 5-year progression (≥T2)-free survival (60 Vs. 82.5%, p = 0.002), 5-year disease-specific survival (73 Vs. 92.5%, p = 0.0004), and overall survival (66 Vs. 89.5%, 0.05).
A patient with variant bladder cancer treated with intravesical immunotherapy has a 27% chance of dying from this disease within 5 years compared to 7.5% chance for a patient with conventional high-grade UC.
高级别尿路上皮癌(UC)常显示出变异分化灶。关于这些变异型尿路上皮肿瘤对卡介苗(BCG)免疫治疗的反应,文献中的信息有限。我们比较了含有腺性、鳞状、巢状和微乳头型分化的UC对BCG治疗的反应与传统非肌层浸润性高级别UC的反应。
1995年6月至2013年12月期间,共有100例患者被诊断为组织学变异型尿路上皮癌。经二次活检确诊为Ta或T1期的41例患者接受了BCG免疫治疗。该组中14例患者为微乳头分化,13例为鳞状分化,9例为腺性分化,7例为巢状变异型。对照组包括140例传统高级别UC患者。两组的治疗和随访方式相似。
变异型肿瘤患者与传统疾病患者具有相似的临床特征,包括年龄、男女比例、分期、Tis的存在情况以及中位随访时间。与传统高级别UC患者相比,变异型肿瘤患者的预后明显更差,包括5年无复发生存率(63.5%对71.5%,p = 0.05)、5年无进展(≥T2)生存率(60%对82.5%,p = 0.002)、5年疾病特异性生存率(73%对92.5%,p = 0.0004)和总生存率(66%对89.5%,p = 0.05)。
接受膀胱内免疫治疗的变异型膀胱癌患者在5年内死于该病的几率为27%,而传统高级别UC患者的这一几率为7.5%。