Zeng Wu-Tao, Liu Zhi-Hao, Li Zhu-Yu, Zhang Ming, Cheng Yun-Jiu
From the Department of Cardiology (W-TZ, Y-JC), the Eastern Hospital of the First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, China; Department of Emergency (Z-HL), the First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, China; Department of Obstetrics and Gynecology (Z-YL), the First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, China; Department of Cardiology (MZ), Beijing Anzhen Hospital, Capital Medical University, Beijing, China.
Medicine (Baltimore). 2016 Mar;95(12):e2949. doi: 10.1097/MD.0000000000002949.
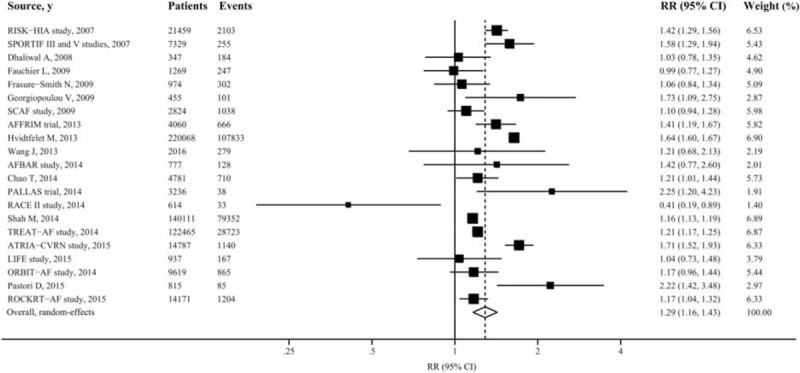
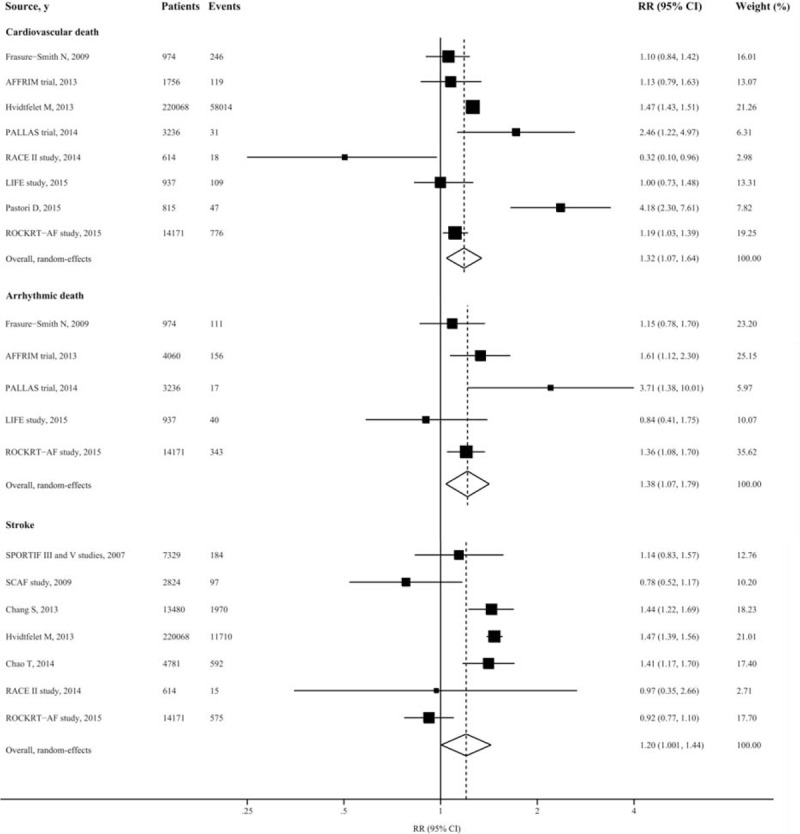
Digoxin has long been used for rate control in atrial fibrillation (AF); its safety remains controversial.We performed a literature search using MEDLINE (source PubMed, January 1, 1966, to July 31, 2015) and EMBASE (January 1, 1980, to July 31, 2015) with no restrictions. Studies that reported relative risk (RR) estimates with 95% confidence intervals (CIs) for the associations of interest were included. Pooled effect estimates were obtained by using random-effects meta-analysis.Twenty-two studies involving 586,594 patients were identified. Patients taking digoxin, as compared with those who took no digoxin, experienced an increased risk of death from any cause (RR: 1.29[95% CI 1.16-1.43]), even after reported adjustment for propensity scores (RR: 1.28[95% CI 1.18-1.39]). The risk of death was increased with patients with or without heart failure (RR: 1.12[95% CI 1.02-1.23] and RR: 1.26[95% CI 1.15-1.29], respectively), and patients taking or not taking beta blockers (RR: 1.17 [95% CI 1.06-1.30] and RR: 1.28 [95% CI 1.08-1.51], respectively). Digoxin use was also associated with increased risk of cardiovascular death (RR: 1.32 [95% CI 1.07-1.64]), arrhythmic death (RR: 1.38 [95% CI 1.07-1.79]), and stroke (RR: 1.20 [95% CI 1.004-1.44]). Digoxin treatment is associated with an absolute risk increase of 19 (95% CI 13-26) additional deaths from any cause per 1000 person-years.Digoxin use is associated with a significant increased risk for death from any cause in patients with AF. This finding suggests a need for reconsideration of present treatment recommendations on use of digoxin in AF.
地高辛长期以来一直用于控制房颤(AF)的心率;其安全性仍存在争议。我们使用MEDLINE(来源为PubMed,1966年1月1日至2015年7月31日)和EMBASE(1980年1月1日至2015年7月31日)进行了无限制的文献检索。纳入了报告了感兴趣关联的相对风险(RR)估计值及95%置信区间(CI)的研究。通过随机效应荟萃分析获得合并效应估计值。共确定了22项涉及586,594例患者的研究。与未服用地高辛的患者相比,服用地高辛的患者全因死亡风险增加(RR:1.29[95%CI 1.16 - 1.43]),即使在报告了倾向评分调整后(RR:1.28[95%CI 1.18 - 1.39])。无论有无心力衰竭患者的死亡风险均增加(RR分别为:1.12[95%CI 1.02 - 1.23]和RR:1.26[95%CI 1.15 - 1.29]),服用或未服用β受体阻滞剂的患者也是如此(RR分别为:1.17 [95%CI 1.06 - 1.30]和RR:1.28 [95%CI 1.08 - 1.51])。使用地高辛还与心血管死亡风险增加(RR:1.32 [95%CI 1.07 - 1.64])、心律失常性死亡风险增加(RR:1.38 [95%CI 1.07 - 1.79])和中风风险增加(RR:1.20 [95%CI 1.004 - 1.44])相关。地高辛治疗每1000人年全因死亡绝对风险增加19例(95%CI 13 - 26)。使用地高辛与房颤患者全因死亡风险显著增加相关。这一发现提示需要重新考虑目前关于房颤患者使用地高辛的治疗建议。