Division of Hematology and Medical Oncology, Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea.
Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
Cancer Res Treat. 2016 Oct;48(4):1373-1381. doi: 10.4143/crt.2015.475. Epub 2016 Mar 23.
The purpose of this study is to investigate the prognostic value of lymph node (LN) ratio (LNR) in patients with breast cancer after neoadjuvant chemotherapy.
This retrospective analysis is based on the data of 814 patientswith stage II/III breast cancer treated with four cycles of doxorubicin/cyclophosphamide followed by four cycles of docetaxel before surgery. We evaluated the clinical significance of LNR (3 categories: low 0-0.20 vs. intermediate 0.21-0.65 vs. high 0.66-1.00) using a Cox proportional regression model.
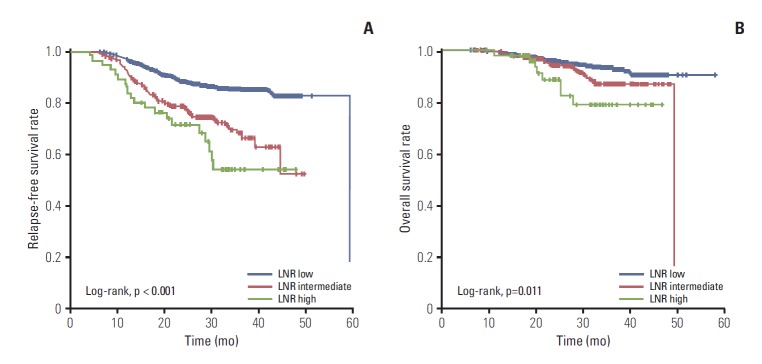
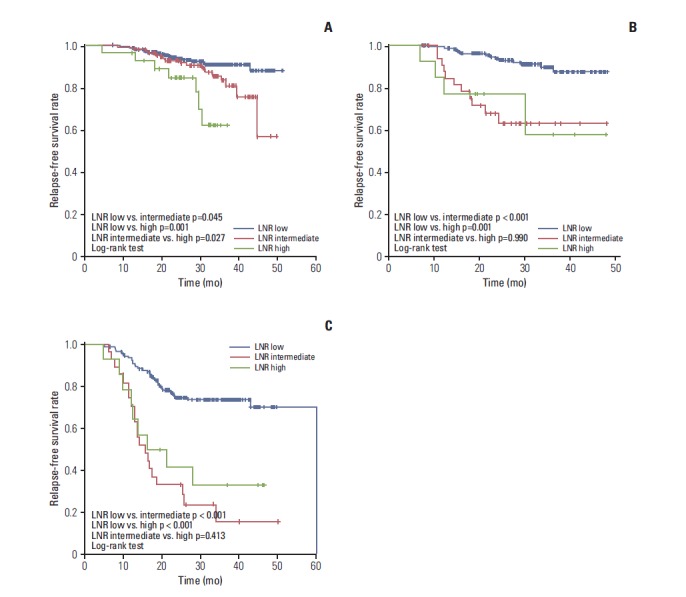
A total of 799 patients underwent breast surgery. Pathologic complete response (pCR, ypT0/isN0) was achieved in 129 patients (16.1%) (hormone receptor [HR] +/human epidermal growth factor receptor 2 [HER2] -, 34/373 [9.1%]; HER2+, 45/210 [21.4%]; triple negative breast cancer, 50/216 [23.1%]). The mean numbers of involved LN and retrieved LN were 2.70 (range, 0 to 42) and 13.98 (range, 1 to 64), respectively. The mean LNR was 0.17 (low, 574 [71.8%]; intermediate, 170 [21.3%]; high, 55 [6.9%]). In univariate analysis, LNR showed significant association with a worse relapse-free survival (3-year relapse-free survival rate 84.8% in low vs. 66.2% in intermediate vs. 54.3% in high; p < 0.001, log-rank test). In multivariate analysis, LNR did not show significant association with recurrence after adjusting for other clinical factors (age, histologic grade, subtype, ypT stage, ypN stage, lymphatic or vascular invasion, and pCR). In subgroup analysis, the LNR system had good prognostic value in HR+/HER2-subtype.
LNR is not superior to ypN stage in predicting clinical outcome of breast cancer after neoadjuvant chemotherapy. However, the prognostic value of the LNR system in HR+/HER2-patients is notable and worthy of further investigation.
本研究旨在探讨新辅助化疗后乳腺癌患者淋巴结比率(LNR)的预后价值。
本回顾性分析基于 814 例接受 4 周期多柔比星/环磷酰胺和 4 周期多西他赛新辅助化疗后行手术治疗的 II/III 期乳腺癌患者的数据。我们使用 Cox 比例风险回归模型评估 LNR(3 个类别:低 0-0.20 vs. 中 0.21-0.65 vs. 高 0.66-1.00)的临床意义。
共有 799 例患者接受了乳房手术。129 例(16.1%)(激素受体[HR]+/人表皮生长因子受体 2 [HER2]-,34/373 [9.1%];HER2+,45/210 [21.4%];三阴性乳腺癌,50/216 [23.1%])达到病理完全缓解(ypT0/isN0)。受累淋巴结和检出淋巴结的平均数量分别为 2.70(范围 0 至 42)和 13.98(范围 1 至 64)。LNR 的平均值为 0.17(低 574 [71.8%];中 170 [21.3%];高 55 [6.9%])。单因素分析显示,LNR 与无复发生存率显著相关(低 LNR 组 3 年无复发生存率为 84.8%,中 LNR 组为 66.2%,高 LNR 组为 54.3%;p<0.001,对数秩检验)。多因素分析显示,在调整其他临床因素(年龄、组织学分级、亚型、ypT 分期、ypN 分期、淋巴管或血管侵犯和 pCR)后,LNR 与复发无显著相关性。在亚组分析中,LNR 系统在 HR+/HER2-亚型中具有良好的预后价值。
LNR 在预测新辅助化疗后乳腺癌患者的临床结局方面并不优于 ypN 分期。然而,LNR 系统在 HR+/HER2-患者中的预后价值值得进一步研究。