Kristensen Morten T, Holm Gitte, Krasheninnikoff Michael, Jensen Pia S, Gebuhr Peter
a Physical Medicine and Rehabilitation Research - Copenhagen (PMR-C) , Department of Physical Therapy ;
b Department of Orthopedic Surgery ;
Acta Orthop. 2016 Jun;87(3):306-11. doi: 10.3109/17453674.2016.1167524. Epub 2016 Apr 18.
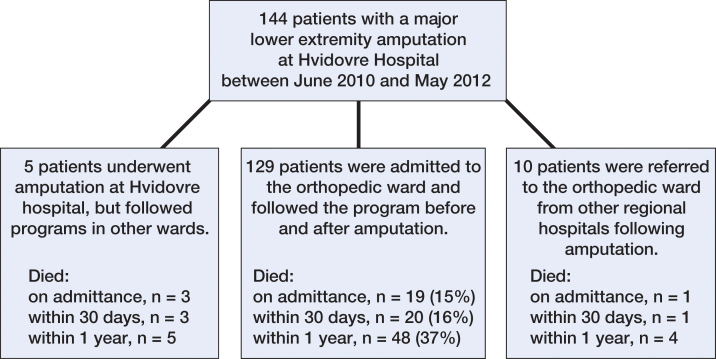
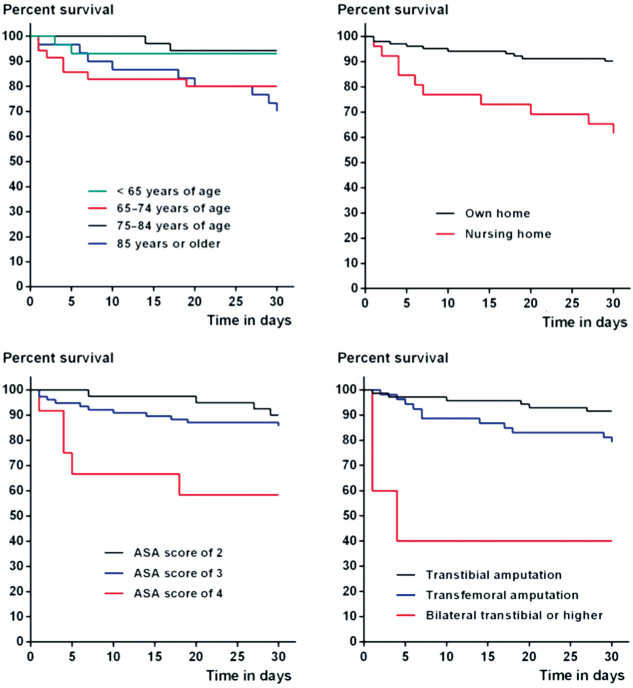
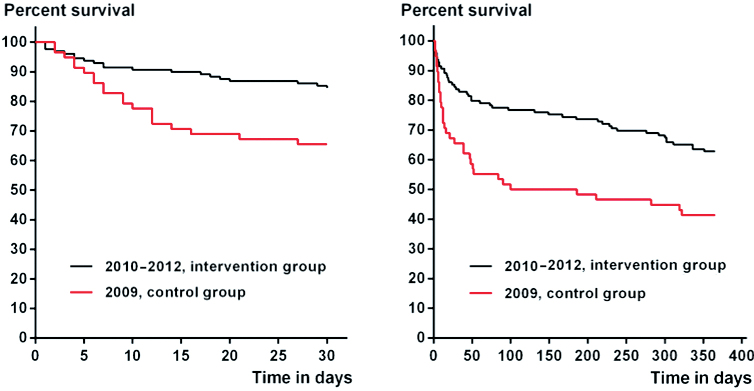
Background and purpose - Historically, high 30-day and 1-year mortality post-amputation rates (> 30% and 50%, respectively) have been reported in patients with a transtibial or higher non-traumatic lower extremity amputation (LEA). We evaluated whether allocating experienced staff and implementing an enhanced, multidisciplinary recovery program would reduce the mortality rates. We also determined factors that influenced mortality rates. Patients and methods - 129 patients with a LEA were consecutively included over a 2-year period, and followed after admission to an acute orthopedic ward. Mortality was compared with historical and concurrent national controls in Denmark. Results - The 30-day and 1-year mortality rates were 16% and 37%, respectively, in the intervention group, as compared to 35% and 59% in the historical control group treated in the same orthopedic ward. Cox proportional harzards models adjusted for age, sex, residential and health status, the disease that caused the amputation, and the index amputation level showed that 30-day and 1-year mortality risk was reduced by 52% (HR =0.48, 95% CI: 0.25-0.91) and by 46% (HR =0.54, 95% CI: 0.35-0.86), respectively, in the intervention group. The risk of death was increased for patients living in a nursing home, for patients with a bilateral LEA, and for patients with low health status. Interpretation - With similarly frail patient groups and instituting an enhanced program for patients after LEA, the risks of death by 30 days and by 1 year after LEA were markedly reduced after allocating staff with expertise.
背景与目的——据历史报道,经胫或更高部位非创伤性下肢截肢(LEA)患者的30天和1年死亡率较高(分别>30%和50%)。我们评估了分配经验丰富的工作人员并实施强化的多学科康复计划是否会降低死亡率。我们还确定了影响死亡率的因素。患者与方法——在2年期间连续纳入129例LEA患者,并在入住急性骨科病房后进行随访。将死亡率与丹麦的历史对照和同期全国对照进行比较。结果——干预组的30天和1年死亡率分别为16%和37%,而在同一骨科病房接受治疗的历史对照组分别为35%和59%。经年龄、性别、居住和健康状况、导致截肢的疾病以及首次截肢水平校正的Cox比例风险模型显示,干预组的30天和1年死亡风险分别降低了52%(HR =0.48,95%CI:0.25 - 0.91)和46%(HR =0.54,95%CI:0.35 - 0.86)。住在养老院的患者、双侧LEA患者以及健康状况较差的患者死亡风险增加。解读——在患者群体同样脆弱的情况下,为LEA患者制定强化计划,在分配专业工作人员后,LEA后30天和1年的死亡风险显著降低。