Saleem Moin A, Kobayashi Yasuko
Paediatric Renal Medicine, University of Bristol, Bristol, UK; Children's Renal Unit, Bristol Royal Hospital for Children, Bristol, UK.
Paediatric Renal Medicine, University of Bristol, Bristol, UK; Department of Pediatrics, Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan.
F1000Res. 2016 Mar 30;5. doi: 10.12688/f1000research.7300.1. eCollection 2016.
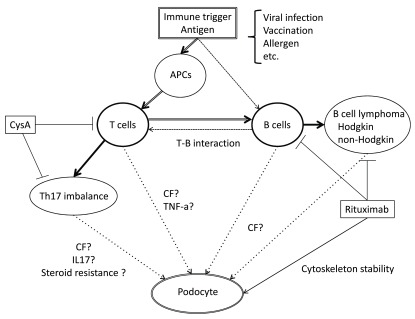
Minimal change disease (MCD) is an important cause of nephrotic syndrome and is characterized by massive proteinuria and hypoalbuminemia, resulting in edema and hypercholesterolemia. The podocyte plays a key role in filtration and its disruption results in a dramatic loss of function leading to proteinuria. Immunologic disturbance has been suggested in the pathogenesis of MCD. Because of its clinical features, such as recurrent relapse/remission course, steroid response in most patients, and rare familial cases, a genetic defect has been thought to be less likely in MCD. Recent progress in whole-exome sequencing reveals pathogenic mutations in familial cases in steroid-sensitive nephrotic syndrome (SSNS) and sheds light on possible mechanisms and key molecules in podocytes in MCD. On the other hand, in the majority of cases, the existence of circulating permeability factors has been implicated along with T lymphocyte dysfunction. Observations of benefit with rituximab added B cell involvement to the disease. Animal models are unsatisfactory, and the humanized mouse may be a good model that well reflects MCD pathophysiology to investigate suggested "T cell dysfunction" directly related to podocytes in vivo. Several candidate circulating factors and their effects on podocytes have been proposed but are still not sufficient to explain whole mechanisms and clinical features in MCD. Another circulating factor disease is focal segmental glomerulosclerosis (FSGS), and it is not clear if this is a distinct entity, or on the same spectrum, implicating the same circulating factor(s). These patients are mostly steroid resistant and often have a rapid relapse after transplantation. In clinical practice, predicting relapse or disease activity and response to steroids is important and is an area where novel biomarkers can be developed based on our growing knowledge of podocyte signaling pathways. In this review, we discuss recent findings in genetics and podocyte biology in MCD.
微小病变病(MCD)是肾病综合征的重要病因,其特征为大量蛋白尿和低白蛋白血症,导致水肿和高胆固醇血症。足细胞在滤过过程中起关键作用,其破坏会导致功能急剧丧失,进而引发蛋白尿。免疫紊乱被认为与MCD的发病机制有关。由于其临床特征,如复发/缓解病程、大多数患者对类固醇有反应以及罕见的家族病例,人们认为MCD发生遗传缺陷的可能性较小。全外显子测序的最新进展揭示了类固醇敏感性肾病综合征(SSNS)家族病例中的致病突变,并阐明了MCD中足细胞的可能机制和关键分子。另一方面,在大多数病例中,循环通透性因子的存在与T淋巴细胞功能障碍有关。利妥昔单抗治疗有效的观察结果提示B细胞也参与了该疾病。动物模型并不理想,人源化小鼠可能是一个很好的模型,能够很好地反映MCD的病理生理学,从而直接在体内研究与足细胞直接相关的“T细胞功能障碍”。已经提出了几种候选循环因子及其对足细胞的影响,但仍不足以解释MCD的整个机制和临床特征。另一种循环因子相关疾病是局灶节段性肾小球硬化(FSGS),目前尚不清楚它是否是一个独立的实体,还是与MCD在同一谱系上,涉及相同的循环因子。这些患者大多对类固醇耐药,移植后常迅速复发。在临床实践中,预测复发或疾病活动以及对类固醇的反应很重要,并且基于我们对足细胞信号通路不断增长的认识,这是一个可以开发新型生物标志物的领域。在这篇综述中,我们讨论了MCD在遗传学和足细胞生物学方面的最新发现。