McAdoo Stephen P, Bedi Rachna, Tarzi Ruth, Griffith Megan, Pusey Charles D, Cairns Thomas D
Vasculitis Centre, Imperial College Healthcare NHS Trust Renal and Vascular Inflammation Section, Department of Medicine, Imperial College London, Hammersmith Hospital, London, UK
Vasculitis Centre, Imperial College Healthcare NHS Trust.
Rheumatology (Oxford). 2016 Aug;55(8):1437-42. doi: 10.1093/rheumatology/kew199. Epub 2016 Apr 19.
B cell depletion is an effective treatment strategy in ANCA-associated vasculitis (AAV). Ofatumumab is a fully humanized anti-CD20 mAb that has shown efficacy in the treatment of haematological malignancy and RA. The use of ofatumumab in the treatment of AAV has not previously been reported.
This study was based on a case series of eight patients who received ofatumumab, in conjunction with low-dose CYC and oral steroids, in the treatment of AAV.
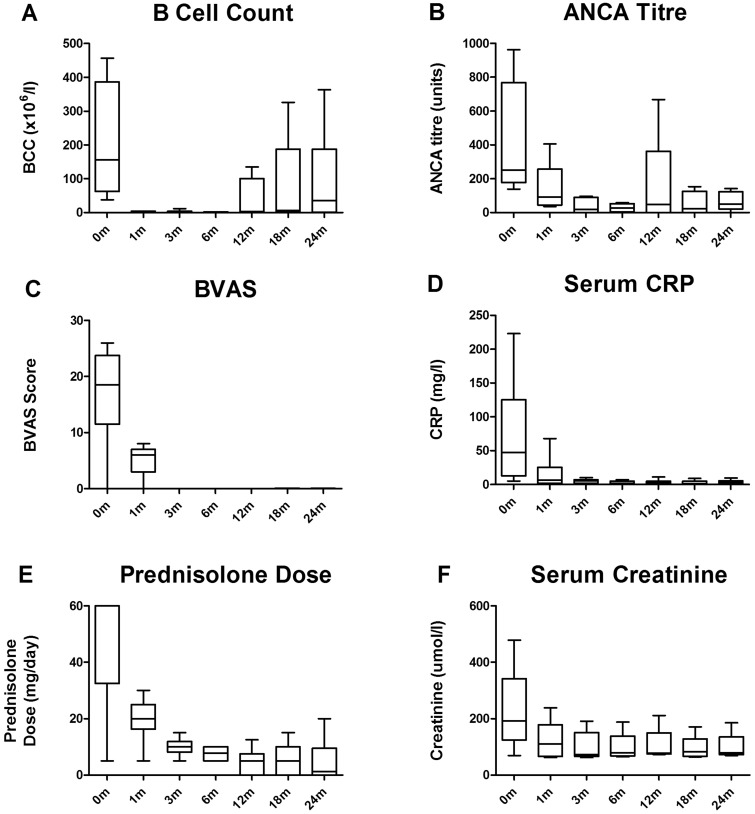
Eight patients received ofatumumab: seven for remission induction in active disease (three relapsing; four with new disease) and one for remission maintenance. B cell depletion was achieved in all patients by 1 month, and was sustained for at least 6 months. All patients with active disease achieved clinical remission (BVAS of zero, or BVAS ⩽5 if all scores due to persistent urinary abnormalities in the presence of stable or improving renal function) by 3 months. This was associated with a rapid fall in ANCA titres, reduced inflammatory responses and improvements in renal function. At 12 months, three patients had repopulated B cells associated with the recurrence of circulating ANCAs, although no patients experienced major clinical relapse in the first 24 months. No unexpected side effects were observed.
Treatment with ofatumumab resulted in similar serological and clinical responses to those seen in previous cohorts treated at our centre with a comparable CS, CYC and rituximab-based regimen. Ofatumumab should be considered an alternative B cell depleting agent in patients who are intolerant of, or unresponsive to, rituximab.
B细胞耗竭是抗中性粒细胞胞浆抗体相关性血管炎(AAV)的一种有效治疗策略。奥法木单抗是一种全人源化抗CD20单克隆抗体,已在血液系统恶性肿瘤和类风湿关节炎的治疗中显示出疗效。此前尚未有关于奥法木单抗治疗AAV的报道。
本研究基于8例接受奥法木单抗联合小剂量环磷酰胺(CYC)及口服糖皮质激素治疗AAV的病例系列。
8例患者接受了奥法木单抗治疗:7例用于诱导活动期疾病缓解(3例复发;4例新发疾病),1例用于维持缓解。所有患者在1个月时均实现了B细胞耗竭,并持续至少6个月。所有活动期疾病患者在3个月时均实现了临床缓解(BVAS为零,或在肾功能稳定或改善的情况下,若所有评分均因持续性尿液异常导致,则BVAS≤5)。这与抗中性粒细胞胞浆抗体滴度迅速下降、炎症反应减轻及肾功能改善相关。在12个月时,3例患者出现B细胞重新增殖并伴有循环抗中性粒细胞胞浆抗体复发,尽管在前24个月内无患者发生主要临床复发。未观察到意外的副作用。
奥法木单抗治疗产生的血清学和临床反应与本中心先前使用类似的环磷酰胺、CYC及基于利妥昔单抗方案治疗的队列相似。对于不耐受利妥昔单抗或对其无反应的患者,应考虑将奥法木单抗作为一种替代性B细胞耗竭剂。