Bould Helen, De Stavola Bianca, Magnusson Cecilia, Micali Nadia, Dal Henrik, Evans Jonathan, Dalman Christina, Lewis Glyn
Department of Psychiatry, University of Oxford, Warneford Hospital, Oxford, UK, Centre for Academic Mental Health, School of Social and Community Medicine, University of Bristol, Bristol, UK
Centre for Statistical Methodology, London School of Hygiene and Tropical Medicine, London, UK.
Int J Epidemiol. 2016 Apr;45(2):480-8. doi: 10.1093/ije/dyw037. Epub 2016 Apr 20.
Clinical anecdote suggests that rates of eating disorders (ED) vary between schools. Given their high prevalence and mortality, understanding risk factors is important. We hypothesised that rates of ED would vary between schools, and that school proportion of female students and proportion of parents with post-high school education would be associated with ED, after accounting for individual characteristics.
Multilevel analysis of register-based, record-linkage data on 55 059 females born in Stockholm County, Sweden, from 1983, finishing high school in 2002-10. Outcome was clinical diagnosis of an ED, or attendance at a specialist ED clinic, aged 16-20 years.
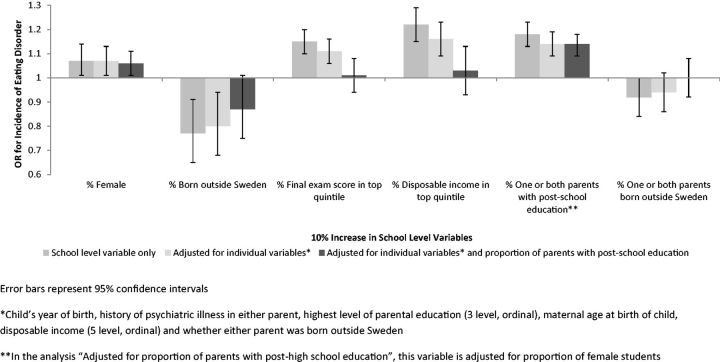
The 5-year cumulative incidence of ED diagnosis aged 16-20 years was 2.4%. Accounting for individual risk factors, with each 10% increase in the proportion of girls at a school, the odds ratio for ED was 1.07 (1.01 to 1.13), P = 0.018. With each 10% increase in the proportion of children with at least one parent with post-high school education, the odds ratio for ED was 1.14 (1.09 to 1.19), P < 0.0001. Predicted probability of an average girl developing an ED was 1.3% at a school with 25% girls where 25% of parents have post-high school education, and 3.3% at a school with 75% girls where 75% of parents have post-high school education.
Rates of ED vary between schools; this is not explained by individual characteristics. Girls at schools with high proportions of female students, and students with highly educated parents, have higher odds of ED regardless of individual risk factors.
临床轶事表明,饮食失调(ED)的发生率在不同学校之间存在差异。鉴于其高患病率和死亡率,了解风险因素很重要。我们假设,在考虑个体特征后,饮食失调的发生率在不同学校之间会有所不同,并且学校女生比例和拥有高中后教育程度的家长比例与饮食失调有关。
对瑞典斯德哥尔摩县1983年出生、2002 - 2010年完成高中学业的55059名女性基于登记册的记录链接数据进行多水平分析。结局是16 - 20岁时饮食失调的临床诊断或在专业饮食失调诊所就诊。
16 - 20岁饮食失调诊断的5年累积发病率为2.4%。考虑个体风险因素后,学校女生比例每增加10%,饮食失调的优势比为1.07(1.01至1.13),P = 0.018。至少有一位家长拥有高中后教育程度的儿童比例每增加10%,饮食失调的优势比为1.14(1.09至1.19),P < 0.0001。在女生占25%且25%的家长拥有高中后教育程度的学校,普通女孩患饮食失调的预测概率为1.3%;在女生占75%且75%的家长拥有高中后教育程度的学校,这一概率为3.3%。
饮食失调的发生率在不同学校之间存在差异;这不能用个体特征来解释。无论个体风险因素如何,女生比例高的学校的女生以及家长受教育程度高的学生患饮食失调的几率更高。