Yamada Ryotaro, Tremmel Jennifer A, Tanaka Shigemitsu, Lin Shin, Kobayashi Yuhei, Hollak M Brooke, Yock Paul G, Fitzgerald Peter J, Schnittger Ingela, Honda Yasuhiro
Division of Cardiovascular Medicine, Stanford Cardiovascular Institute, Stanford University School of Medicine, Stanford, CA.
Division of Cardiovascular Medicine, Stanford Cardiovascular Institute, Stanford University School of Medicine, Stanford, CA
J Am Heart Assoc. 2016 Apr 20;5(4):e001735. doi: 10.1161/JAHA.114.001735.
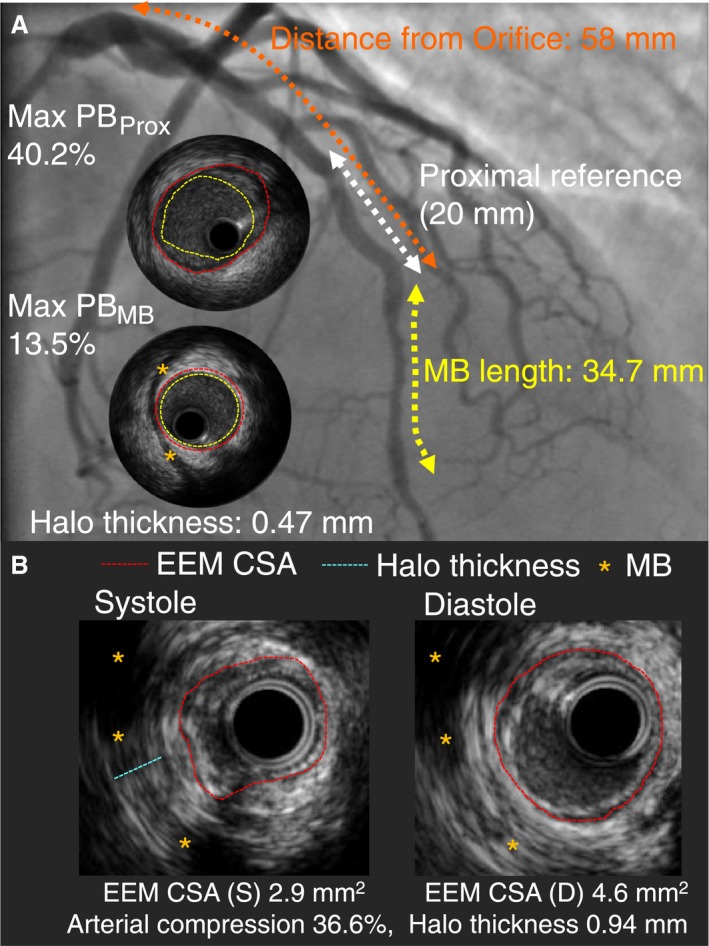
The presence of a myocardial bridge (MB) has been shown to promote atherosclerotic plaque formation proximal to the MB, presumably because of hemodynamic disturbances provoked by retrograde blood flow toward this segment in cardiac systole. We aimed to determine the anatomic and functional properties of an MB related to the extent of atherosclerosis assessed by intravascular ultrasound.
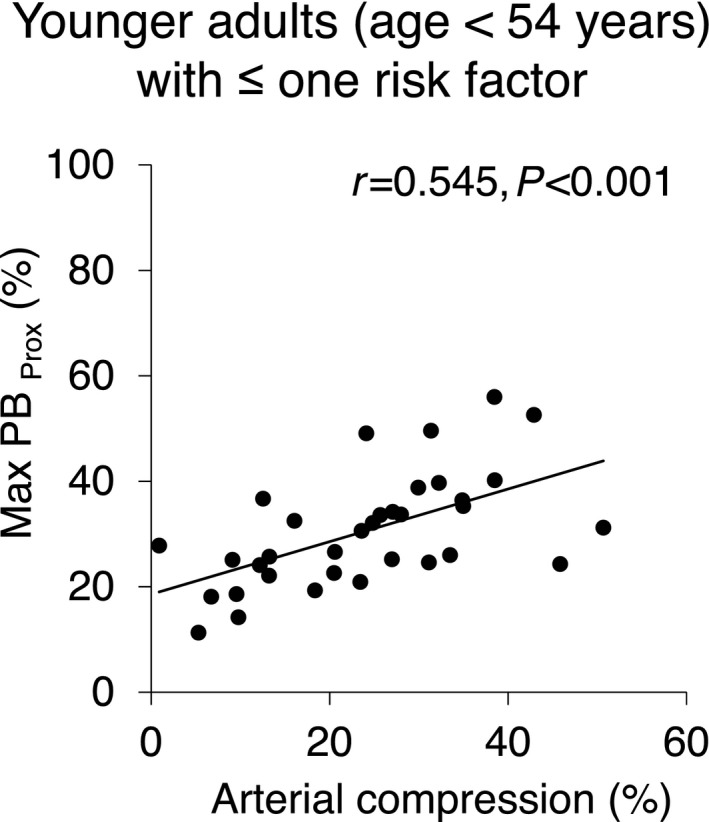
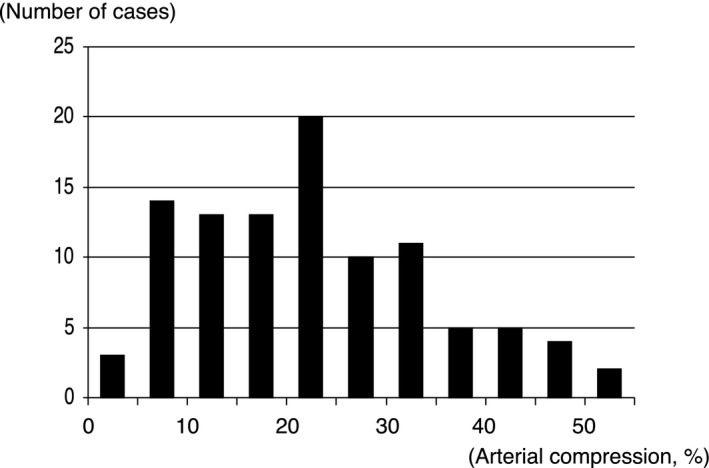
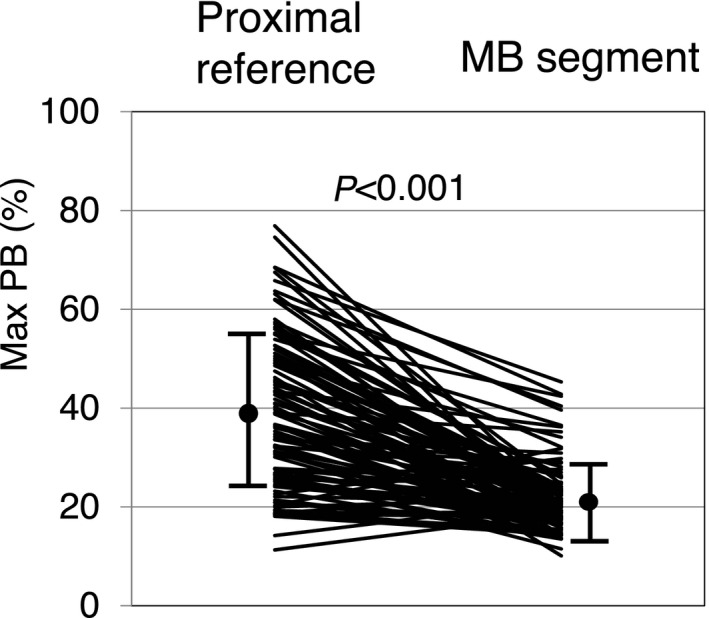
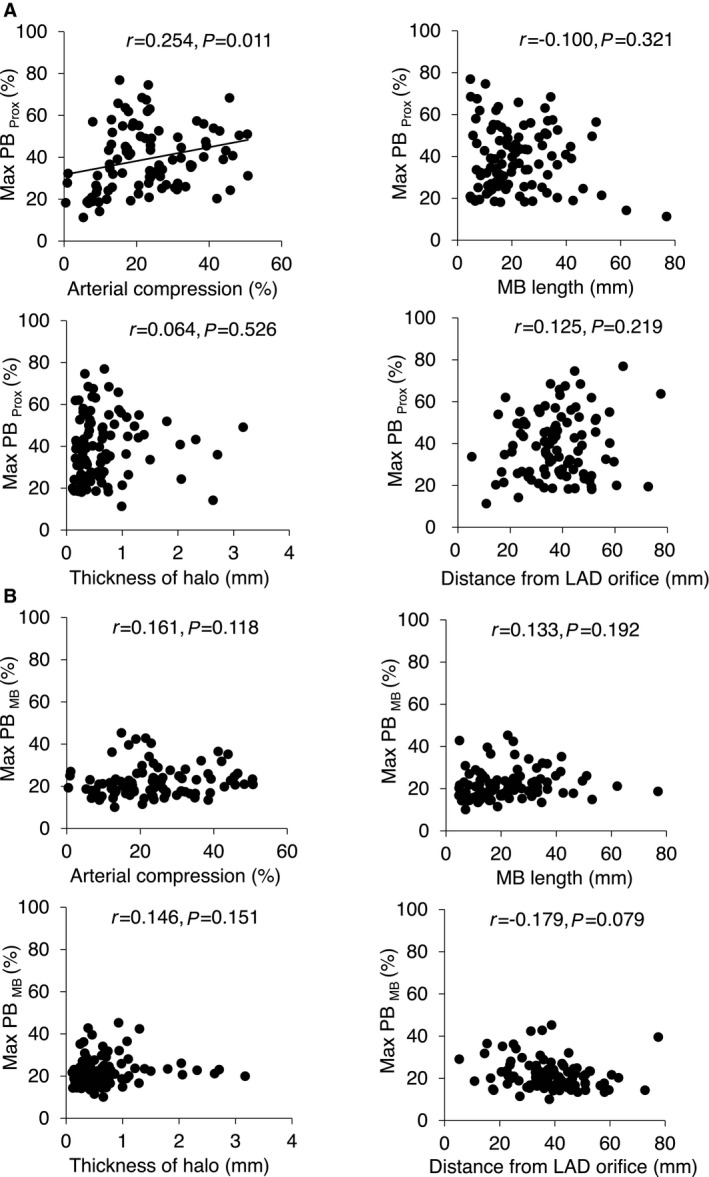
We enrolled 100 patients with angina but no significant obstructive coronary artery disease who had an intravascular ultrasound-detected MB in the left anterior descending artery (median age 54 years, 36% male). The MB was identified with intravascular ultrasound by the presence of an echolucent band (halo). Anatomically, the MB length was 22±13 mm, and halo thickness was 0.7±0.6 mm. Functionally, systolic arterial compression was 23±12%. The maximum plaque burden up to 20 mm proximal to the MB entrance was significantly greater than the maximum plaque burden within the MB segment. Among the intravascular ultrasound-defined MB properties, arterial compression was the sole MB parameter that demonstrated a significant positive correlation with maximum plaque burden up to 20 mm proximal to the MB entrance (r=0.254, P=0.011 overall; r=0.545, P<0.001 low coronary risk). In multivariate analysis, adjusting for clinical characteristics and coronary risk factors, arterial compression was independently associated with maximum plaque burden up to 20 mm proximal to the MB entrance.
In patients with an MB in the left anterior descending artery, the percentage of arterial compression is related directly to the burden of atherosclerotic plaque located proximally to the MB, particularly in patients who otherwise have low coronary risk. This may prove helpful in identifying high-risk MB patients.
心肌桥(MB)的存在已被证明会促进MB近端动脉粥样硬化斑块的形成,推测这是由于心脏收缩期逆向血流冲向该节段所引发的血流动力学紊乱所致。我们旨在确定与血管内超声评估的动脉粥样硬化程度相关的MB的解剖学和功能特性。
我们纳入了100例患有心绞痛但无明显阻塞性冠状动脉疾病的患者,这些患者在左前降支血管内超声检测到有MB(中位年龄54岁,男性占36%)。通过血管内超声发现无回声带(晕)来识别MB。在解剖学上,MB长度为22±13毫米,晕厚度为0.7±0.6毫米。在功能上,收缩期动脉压迫为23±12%。MB入口近端20毫米处的最大斑块负荷显著大于MB节段内的最大斑块负荷。在血管内超声定义的MB特性中,动脉压迫是唯一与MB入口近端20毫米处的最大斑块负荷呈显著正相关的MB参数(总体r=0.254,P=0.011;低冠状动脉风险r=0.545,P<0.001)。在多变量分析中,校正临床特征和冠状动脉危险因素后,动脉压迫与MB入口近端20毫米处的最大斑块负荷独立相关。
在左前降支有MB的患者中,动脉压迫百分比与MB近端的动脉粥样硬化斑块负荷直接相关,特别是在其他方面冠状动脉风险较低的患者中。这可能有助于识别高危MB患者。