Manjunatha R, Pundarikaksha H P, Madhusudhana H R, Amarkumar J, Hanumantharaju B K
Department of Pharmacology, Kempegowda Institute of Medical Sciences, Bengaluru, Karnataka, India.
Department of Urology, Kempegowda Institute of Medical Sciences Hospital and Research Centre, Bengaluru, Karnataka, India.
Indian J Pharmacol. 2016 Mar-Apr;48(2):134-40. doi: 10.4103/0253-7613.178825.
Benign prostatic hyperplasia (BPH) is a common and progressive disease affecting elderly males, often associated with lower urinary tract symptoms (LUTS). α1-blockers are the mainstay in symptomatic therapy of BPH. Because of their greater uroselectivity and minimal hemodynamic effects, alfuzosin, tamsulosin, and silodosin are generally preferred. The aim of this study was to compare the efficacy and tolerability of alfuzosin, tamsulosin, and silodosin in patients with BPH and LUTS.
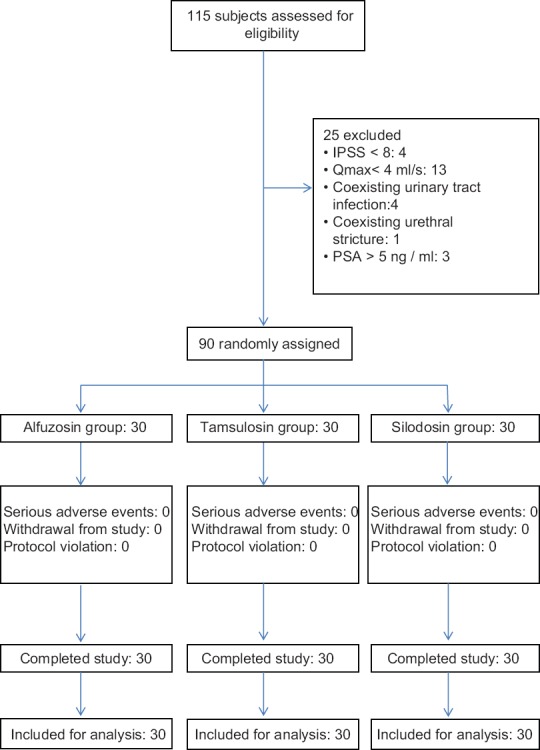
Ninety subjects with BPH and LUTS were randomized into three groups of thirty in each, to receive alfuzosin sustained release (SR) 10 mg, tamsulosin 0.4 mg, or silodosin 8 mg for 12 weeks. The primary outcome measure was a change in the International Prostate Symptom Score (IPSS), and the secondary outcome measures were changes in individual subjective symptom scores, quality of life score (QLS), and peak flow rate (Qmax) from baseline. The treatment response was monitored at 2, 4, 8, and 12 weeks.
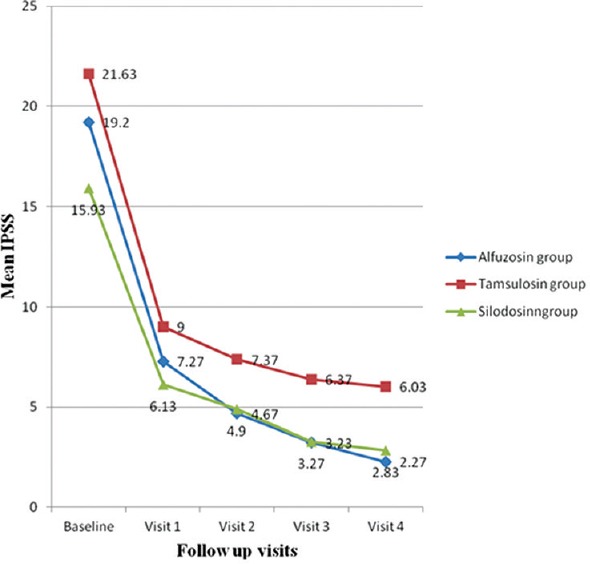
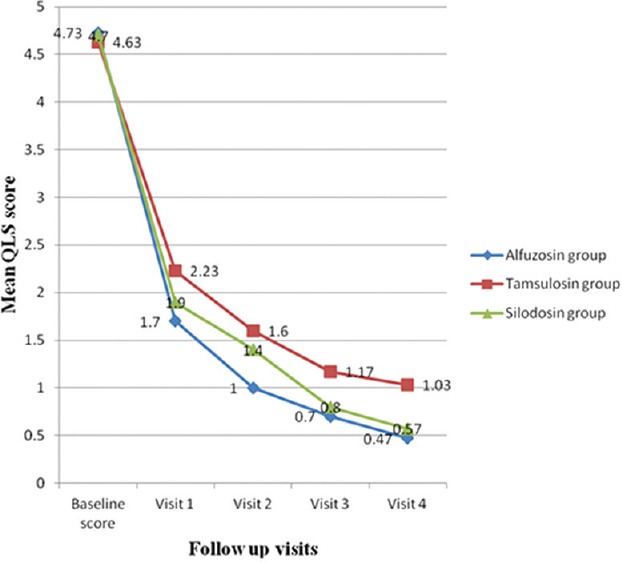
IPSS improved by 88.18%, 72.12%, and 82.23% in alfuzosin SR, tamsulosin and silodosin groups (P < 0.001) at 12 weeks. Improvement in QLS was >75% in all the three groups (P < 0.001). A significant improvement in Qmax was seen with alfuzosin and tamsulosin (P = 0.025 and P < 0.001) but not with silodosin (P = 0.153). However, the intergroup differences in IPSS, QLS, and Qmax were not significant. Ejaculatory dysfunction was more common with silodosin and corrected QT (QTc) prolongation occurred only with alfuzosin (two subjects) and tamsulosin (three subjects).
Alfuzosin, tamsulosin, and silodosin showed similar efficacy in improvement of LUTS secondary to BPH, with good tolerability, acceptability, and minimum hemodynamic adverse effects. Alfuzosin, tamsulosin, and silodosin are comparable in efficacy in symptomatic management of BPH. The occurrence of QTc prolongation in three subjects with tamsulosin in the present study is an unexpected adverse event as there are no reports of QTc prolongation with tamsulosin in any of the previous studies.
良性前列腺增生(BPH)是一种影响老年男性的常见渐进性疾病,常伴有下尿路症状(LUTS)。α1受体阻滞剂是BPH症状性治疗的主要药物。由于其更高的尿道选择性和最小的血流动力学效应,阿夫唑嗪、坦索罗辛和西洛多辛通常更受青睐。本研究的目的是比较阿夫唑嗪、坦索罗辛和西洛多辛在BPH合并LUTS患者中的疗效和耐受性。
90例BPH合并LUTS患者被随机分为三组,每组30例,分别接受阿夫唑嗪缓释片(SR)10mg、坦索罗辛0.4mg或西洛多辛8mg治疗12周。主要结局指标是国际前列腺症状评分(IPSS)的变化,次要结局指标是个体主观症状评分、生活质量评分(QLS)以及与基线相比的最大尿流率(Qmax)的变化。在第2、4、8和12周监测治疗反应。
在12周时,阿夫唑嗪SR组、坦索罗辛组和西洛多辛组的IPSS改善率分别为88.18%、72.12%和82.23%(P<0.001)。三组的QLS改善率均>75%(P<0.001)。阿夫唑嗪和坦索罗辛使Qmax有显著改善(P=0.025和P<0.001),而西洛多辛未使Qmax显著改善(P=0.153)。然而,IPSS、QLS和Qmax的组间差异不显著。射精功能障碍在西洛多辛组更常见,校正QT(QTc)延长仅在阿夫唑嗪组(2例)和坦索罗辛组(3例)出现。
阿夫唑嗪、坦索罗辛和西洛多辛在改善BPH继发的LUTS方面显示出相似的疗效,具有良好的耐受性、可接受性和最小的血流动力学不良反应。阿夫唑嗪、坦索罗辛和西洛多辛在BPH症状管理方面的疗效相当。本研究中坦索罗辛组有3例出现QTc延长,这是一个意外的不良事件,因为之前的任何研究均未报道过坦索罗辛导致QTc延长。