Elke Gunnar, van Zanten Arthur R H, Lemieux Margot, McCall Michele, Jeejeebhoy Khursheed N, Kott Matthias, Jiang Xuran, Day Andrew G, Heyland Daren K
Department of Anaesthesiology and Intensive Care Medicine, University Medical Centre Schleswig-Holstein, Campus Kiel, Arnold-Heller-Str. 3 Haus 12, 24105, Kiel, Germany.
Department of Intensive Care, Gelderse Vallei Hospital, Willy Brandtlaan 10, 6716, RP, Ede, The Netherlands.
Crit Care. 2016 Apr 29;20(1):117. doi: 10.1186/s13054-016-1298-1.
Enteral nutrition (EN) is recommended as the preferred route for early nutrition therapy in critically ill adults over parenteral nutrition (PN). A recent large randomized controlled trial (RCT) showed no outcome differences between the two routes. The objective of this systematic review was to evaluate the effect of the route of nutrition (EN versus PN) on clinical outcomes of critically ill patients.
An electronic search from 1980 to 2016 was performed identifying relevant RCTs. Individual trial data were abstracted and methodological quality of included trials scored independently by two reviewers. The primary outcome was overall mortality and secondary outcomes included infectious complications, length of stay (LOS) and mechanical ventilation. Subgroup analyses were performed to examine the treatment effect by dissimilar caloric intakes, year of publication and trial methodology. We performed a test of asymmetry to assess for the presence of publication bias.
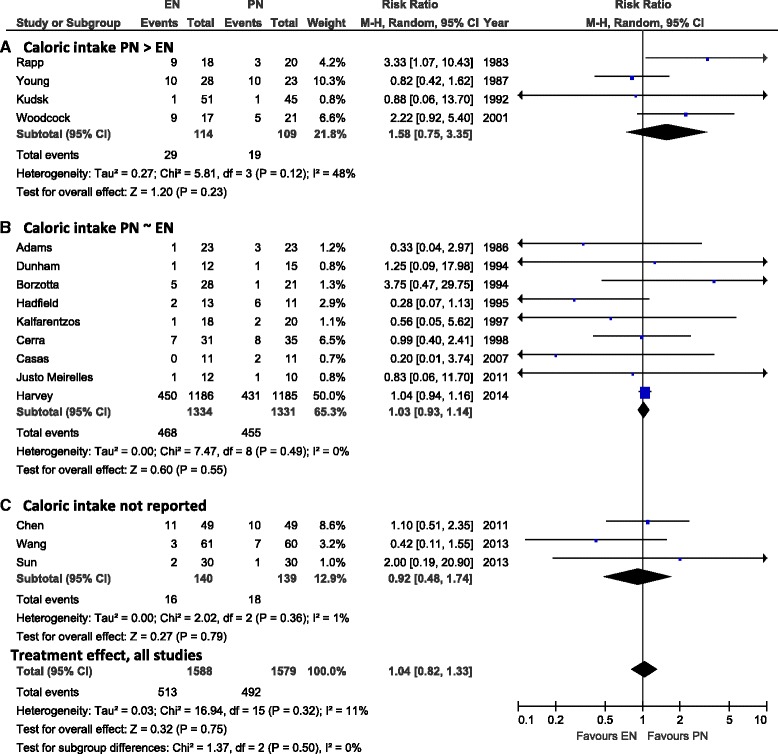
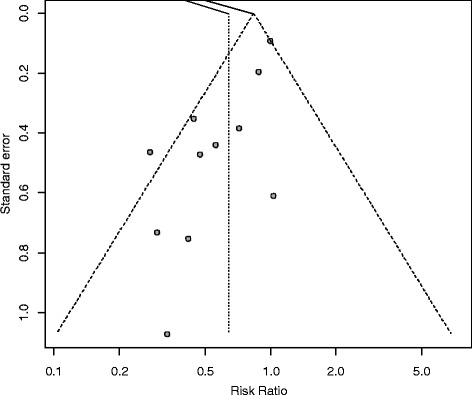
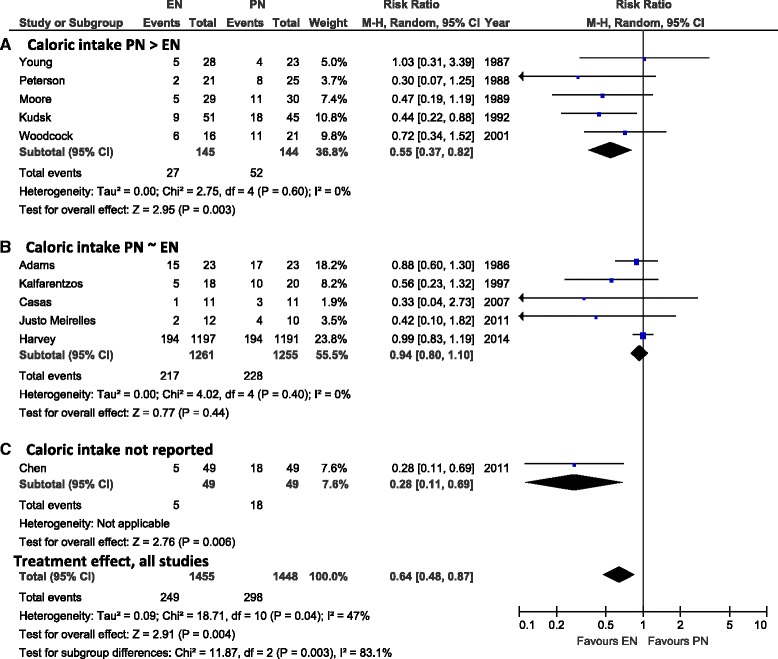
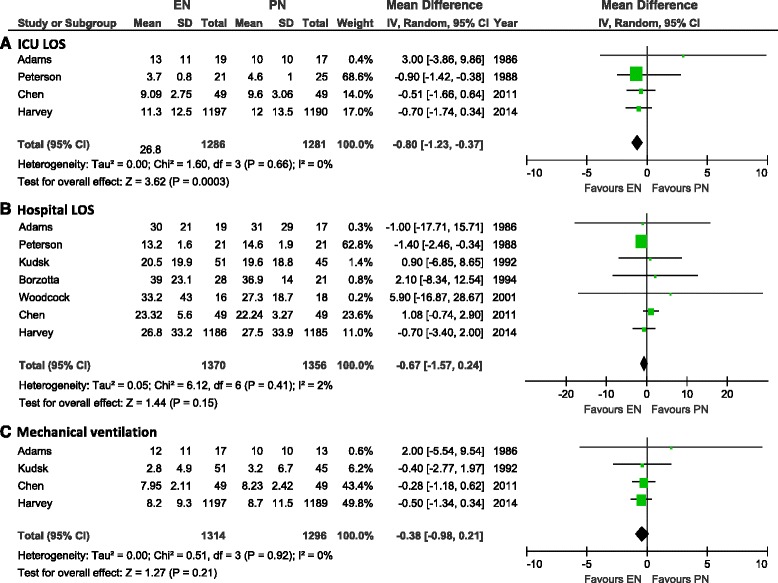
A total of 18 RCTs studying 3347 patients met inclusion criteria. Median methodological score was 7 (range, 2-12). No effect on overall mortality was found (1.04, 95 % CI 0.82, 1.33, P = 0.75, heterogeneity I(2) = 11 %). EN compared to PN was associated with a significant reduction in infectious complications (RR 0.64, 95 % CI 0.48, 0.87, P = 0.004, I(2) = 47 %). This was more pronounced in the subgroup of RCTs where the PN group received significantly more calories (RR 0.55, 95 % CI 0.37, 0.82, P = 0.003, I(2) = 0 %), while no effect was seen in trials where EN and PN groups had a similar caloric intake (RR 0.94, 95 % CI 0.80, 1.10, P = 0.44, I(2) = 0 %; test for subgroup differences, P = 0.003). Year of publication and methodological quality did not influence these findings; however, a publication bias may be present as the test of asymmetry was significant (P = 0.003). EN was associated with significant reduction in ICU LOS (weighted mean difference [WMD] -0.80, 95 % CI -1.23, -0.37, P = 0.0003, I(2) = 0 %) while no significant differences in hospital LOS and mechanical ventilation were observed.
In critically ill patients, the use of EN as compared to PN has no effect on overall mortality but decreases infectious complications and ICU LOS. This may be explained by the benefit of reduced macronutrient intake rather than the enteral route itself.
对于危重症成人患者,肠内营养(EN)被推荐为早期营养治疗的首选途径,优于肠外营养(PN)。最近一项大型随机对照试验(RCT)显示,这两种途径在结局方面并无差异。本系统评价的目的是评估营养途径(EN与PN)对危重症患者临床结局的影响。
进行了一项从1980年至2016年的电子检索,以识别相关的随机对照试验。提取了单个试验数据,两名评价者独立对纳入试验的方法学质量进行评分。主要结局是总体死亡率,次要结局包括感染性并发症、住院时间(LOS)和机械通气。进行亚组分析以检验不同热量摄入、发表年份和试验方法对治疗效果的影响。我们进行了不对称性检验以评估发表偏倚的存在。
共有18项研究3347例患者的随机对照试验符合纳入标准。方法学评分中位数为7分(范围为2 - 12分)。未发现对总体死亡率有影响(1.04,95%可信区间0.82,1.33,P = 0.75,异质性I(2)=11%)。与PN相比,EN与感染性并发症显著减少相关(风险比0.64,95%可信区间0.48,0.87,P = 0.004,I(2)=47%)。在PN组摄入热量显著更多的随机对照试验亚组中,这种情况更为明显(风险比0.55,95%可信区间0.37,0.82,P = 0.003,I(2)=0%),而在EN组和PN组热量摄入相似的试验中未观察到影响(风险比0.94,95%可信区间0.80,1.10,P = 0.44,I(2)=0%;亚组差异检验,P = 0.003)。发表年份和方法学质量并未影响这些结果;然而,由于不对称性检验具有显著性(P = 0.003),可能存在发表偏倚。EN与ICU住院时间显著缩短相关(加权平均差[WMD] -0.80,95%可信区间 -1.23, -0.37,P = 0.0003,I(2)=0%),而在住院时间和机械通气方面未观察到显著差异。
在危重症患者中,与PN相比,使用EN对总体死亡率无影响,但可降低感染性并发症和ICU住院时间。这可能是由于大量营养素摄入量减少的益处而非肠内途径本身所致。