Nakibuuka Jane, Sajatovic Martha, Nankabirwa Joaniter, Ssendikadiwa Charles, Kalema Nelson, Kwizera Arthur, Byakika-Tusiime Jayne, Furlan Anthony J, Kayima James, Ddumba Edward, Katabira Elly
Department of Medicine, School of Medicine, Makerere University College of Health Sciences, Kampala, Uganda.
Department of Medicine, Mulago National referral hospital, Kampala, Uganda.
PLoS One. 2016 May 4;11(5):e0154333. doi: 10.1371/journal.pone.0154333. eCollection 2016.
Integrated care pathways (ICP) in stroke management are increasingly being implemented to improve outcomes of acute stroke patients. We evaluated the effect of implementing a 72 hour stroke care bundle on early outcomes among patients admitted within seven days post stroke to the national referral hospital in Uganda.
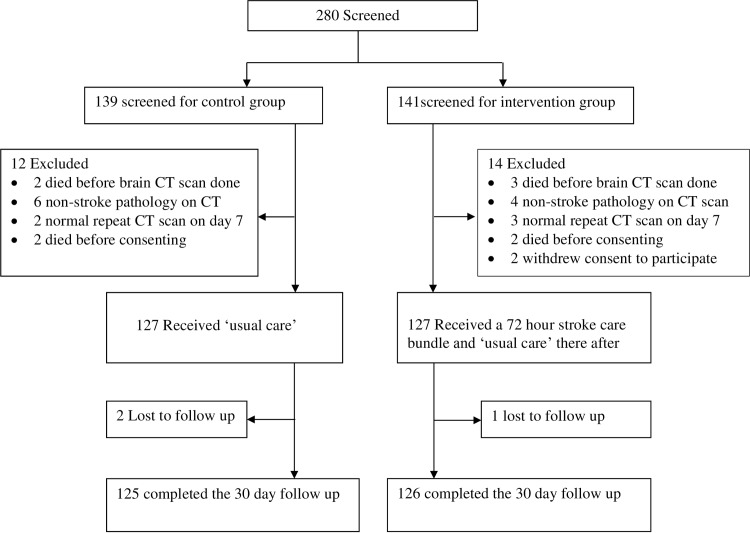
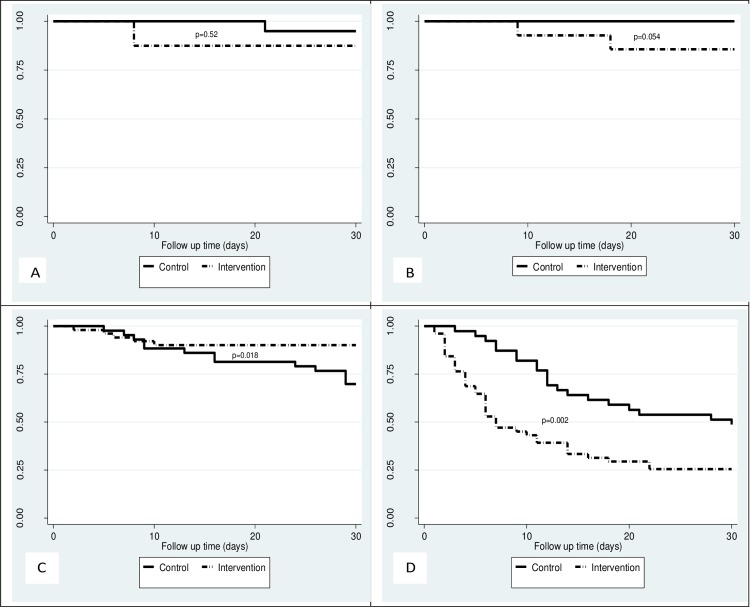
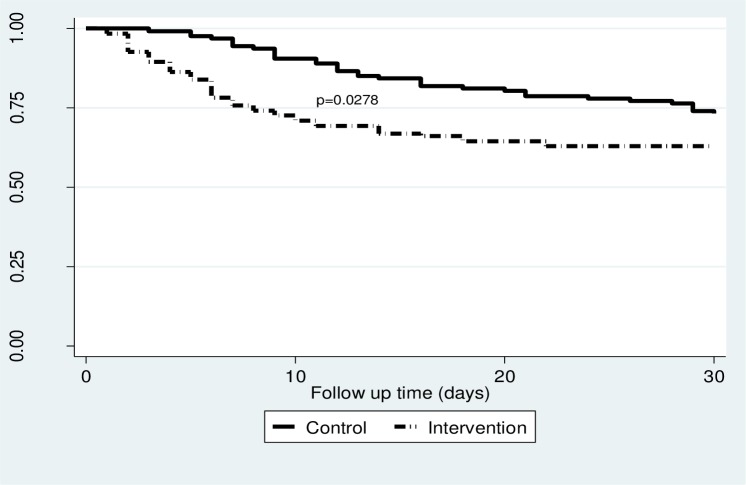
In a one year non-randomised controlled study, 127 stroke patients who had 'usual care' (control group) were compared to 127 stroke patients who received selected elements from an ICP (intervention group). Patients were consecutively enrolled (controls first, intervention group second) into each group over 5 month periods and followed to 30-days post stroke. Incidence outcomes (mortality and functional ability) were compared using chi square test and adjusted for potential confounders. Kaplan Meier survival estimates and log rank test for comparison were used for time to death analysis for all strokes and by stroke severity categories. Secondary outcomes were in-hospital mortality, median survival time and median length of hospital stay.
Mortality within 7 days was higher in the intervention group compared to controls (RR 13.1, 95% CI 3.3-52.9). There was no difference in 30-day mortality between the two groups (RR 1.2, 95% CI 0.5-2.6). There was better 30-day survival in patients with severe stroke in the intervention group compared to controls (P = 0.018). The median survival time was 30 days (IQR 29-30 days) in the control group and 30 days (IQR 7-30 days) in the intervention group. In the intervention group, 41patients (32.3%) died in hospital compared to 23 (18.1%) in controls (P < 0.001). The median length of hospital stay was 8 days (IQR 5-12 days) in the controls and 4 days (IQR 2-7 days) in the intervention group. There was no difference in functional outcomes between the groups (RR 0.9, 95% CI 0.4-2.2).
While implementing elements of a stroke-focused ICP in a Ugandan national referral hospital appeared to have little overall benefit in mortality and functioning, patients with severe stroke may benefit on selected outcomes. More research is needed to better understand how and when stroke protocols should be implemented in sub-Saharan African settings.
Pan African Clinical Trials Registry PACTR201510001272347.
在中风管理中,越来越多地采用综合护理路径(ICP)来改善急性中风患者的治疗效果。我们评估了在乌干达国家转诊医院对中风后7天内入院的患者实施72小时中风护理套餐对早期治疗效果的影响。
在一项为期一年的非随机对照研究中,将127名接受“常规护理”的中风患者(对照组)与127名接受ICP中选定要素的中风患者(干预组)进行比较。在5个月的时间内,患者被连续纳入每组(先纳入对照组,后纳入干预组),并随访至中风后30天。使用卡方检验比较发病率结果(死亡率和功能能力),并对潜在混杂因素进行调整。使用Kaplan Meier生存估计和对数秩检验进行比较,对所有中风患者以及按中风严重程度分类的患者进行死亡时间分析。次要结果包括住院死亡率、中位生存时间和中位住院时间。
干预组7天内的死亡率高于对照组(相对风险13.1,95%置信区间3.3 - 52.9)。两组30天死亡率无差异(相对风险1.2,95%置信区间0.5 - 2.6)。与对照组相比,干预组中重度中风患者的30天生存率更高(P = 0.018)。对照组的中位生存时间为30天(四分位间距29 - 30天),干预组为30天(四分位间距7 - 30天)。在干预组中,41名患者(32.3%)在医院死亡,而对照组为23名(18.1%)(P < 0.001)。对照组的中位住院时间为8天(四分位间距5 - 12天),干预组为4天(四分位间距2 - 7天)。两组之间的功能结果无差异(相对风险0.9,95%置信区间0.4 - 2.2)。
虽然在乌干达国家转诊医院实施以中风为重点的ICP要素在死亡率和功能方面总体益处不大,但重度中风患者在某些选定结果上可能受益。需要更多研究来更好地了解在撒哈拉以南非洲地区应如何以及何时实施中风治疗方案。
泛非临床试验注册中心PACTR201510001272347。