Garg Pankaj, Kidambi Ananth, Foley James R J, Musa Tarique Al, Ripley David P, Swoboda Peter P, Erhayiem Bara, Dobson Laura E, McDiarmid Adam K, Greenwood John P, Plein Sven
Multidisciplinary Cardiovascular Research Centre & Leeds Institute of Cardiovascular and Metabolic Medicine, University of Leeds , Leeds , UK.
Open Heart. 2016 May 2;3(1):e000337. doi: 10.1136/openhrt-2015-000337. eCollection 2016.
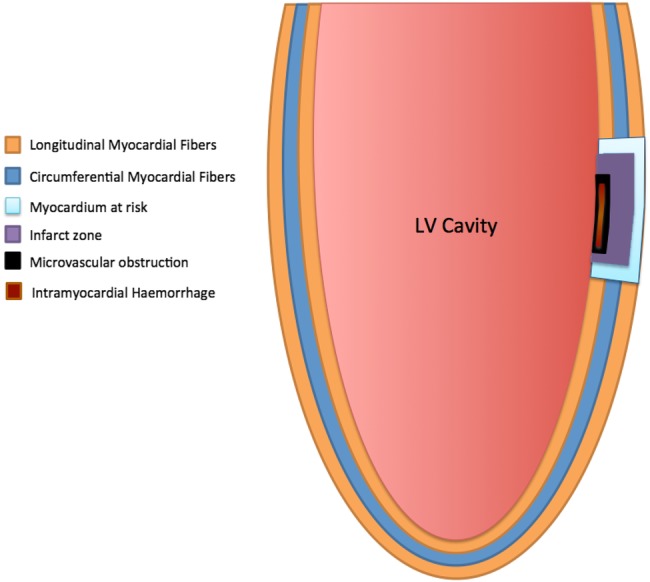
Microvascular obstruction (MVO) and intramyocardial haemorrhage (IMH) are associated with adverse prognosis, independently of infarct size after reperfused ST-elevation myocardial infarction (STEMI). Mitral annular plane systolic excursion (MAPSE) is a well-established parameter of longitudinal function on echocardiography.
We aimed to investigate how acute MAPSE, assessed by a four-chamber cine-cardiovascular MR (CMR), is associated with MVO, IMH and convalescent left ventricular (LV) remodelling.
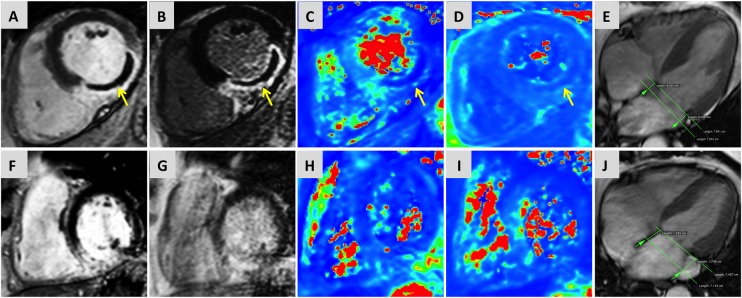
54 consecutive patients underwent CMR at 3T (Intera CV, Philips Healthcare, Best, The Netherlands) within 3 days of reperfused STEMI. Cine, T2-weighted, T2* and late gadolinium enhancement (LGE) imaging were performed. Infarct and MVO extent were measured from LGE images. The presence of IMH was investigated by combined analysis of T2w and T2* images. Averaged-MAPSE (medial-MAPSE+lateral-MAPSE/2) was calculated from 4-chamber cine imaging.
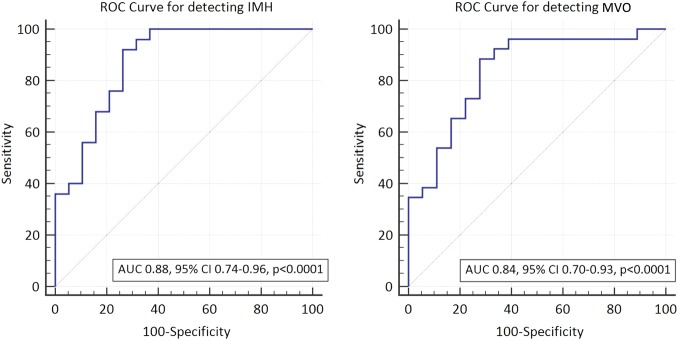
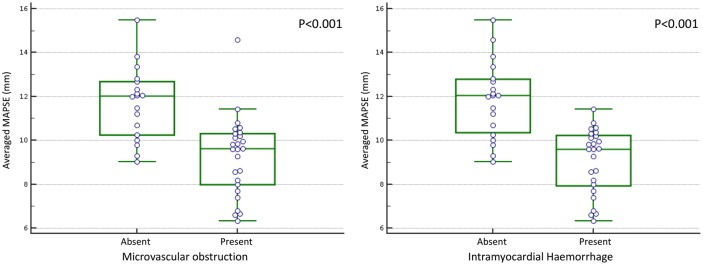
44 patients completed the baseline scan and 38 patients completed 3-month scans. 26 (59%) patients had MVO and 25 (57%) patients had IMH. Presence of MVO and IMH were associated with lower averaged-MAPSE (11.7±0.4 mm vs 9.3±0.3 mm; p<0.001 and 11.8±0.4 mm vs 9.2±0.3 mm; p<0.001, respectively). IMH (β=-0.655, p<0.001) and MVO (β=-0.567, p<0.001) demonstrated a stronger correlation to MAPSE than other demographic and infarct characteristics. MAPSE ≤10.6 mm demonstrated 89% sensitivity and 72% specificity for the detection of MVO and 92% sensitivity and 74% specificity for IMH. LV remodelling in convalescence was not associated with MAPSE (AUC 0.62, 95% CI 0.44 to 0.77, p=0.22).
Postreperfused STEMI, LV longitudinal function assessed by MAPSE can independently predict the presence of MVO and IMH.
微血管阻塞(MVO)和心肌内出血(IMH)与不良预后相关,独立于再灌注ST段抬高型心肌梗死(STEMI)后的梗死面积。二尖瓣环平面收缩期位移(MAPSE)是超声心动图上已确立的纵向功能参数。
我们旨在研究通过四腔电影心血管磁共振成像(CMR)评估的急性MAPSE如何与MVO、IMH和恢复期左心室(LV)重构相关。
54例连续的患者在再灌注STEMI后3天内接受了3T(Intera CV,飞利浦医疗保健公司,荷兰贝斯特)的CMR检查。进行了电影成像、T2加权成像、T2成像和延迟钆增强(LGE)成像。从LGE图像测量梗死和MVO范围。通过T2w和T2图像的联合分析研究IMH的存在情况。从四腔电影成像计算平均MAPSE(内侧MAPSE+外侧MAPSE/2)。
44例患者完成了基线扫描,38例患者完成了3个月的扫描。26例(59%)患者有MVO,25例(57%)患者有IMH。MVO和IMH的存在与较低的平均MAPSE相关(分别为11.7±0.4mm对9.3±0.3mm;p<0.001和11.8±0.4mm对9.2±0.3mm;p<0.001)。与其他人口统计学和梗死特征相比,IMH(β=-0.655,p<0.001)和MVO(β=-0.567,p<0.001)与MAPSE的相关性更强。MAPSE≤10.6mm对MVO检测的敏感性为89%,特异性为72%,对IMH检测的敏感性为92%,特异性为74%。恢复期的LV重构与MAPSE无关(曲线下面积0.62,95%可信区间0.44至0.77,p=0.22)。
再灌注后STEMI,通过MAPSE评估的LV纵向功能可独立预测MVO和IMH的存在。