Leal Maria do Carmo, Esteves-Pereira Ana Paula, Nakamura-Pereira Marcos, Torres Jacqueline Alves, Domingues Rosa Maria Soares Madeira, Dias Marcos Augusto Bastos, Moreira Maria Elizabeth, Theme-Filha Mariza, da Gama Silvana Granado Nogueira
Department of Epidemiology and Quantitative Methods in Health, Sérgio Arouca National School of Public Health, Oswaldo Cruz Foundation, Rio de Janeiro, Brazil.
National Institute of Women, Children and Adolescents Health Fernandes Figueira, Oswaldo Cruz Foundation, Rio de Janeiro, Brazil.
PLoS One. 2016 May 19;11(5):e0155511. doi: 10.1371/journal.pone.0155511. eCollection 2016.
A large proportion of the rise in prematurity worldwide is owing to late preterm births, which may be due to the expansion of obstetric interventions, especially pre-labour caesarean section. Late preterm births pose similar risks to overall prematurity, making this trend a concern. In this study, we describe factors associated with provider-initiated late preterm birth and verify differences in provider-initiated late preterm birth rates between public and private health services according to obstetric risk.
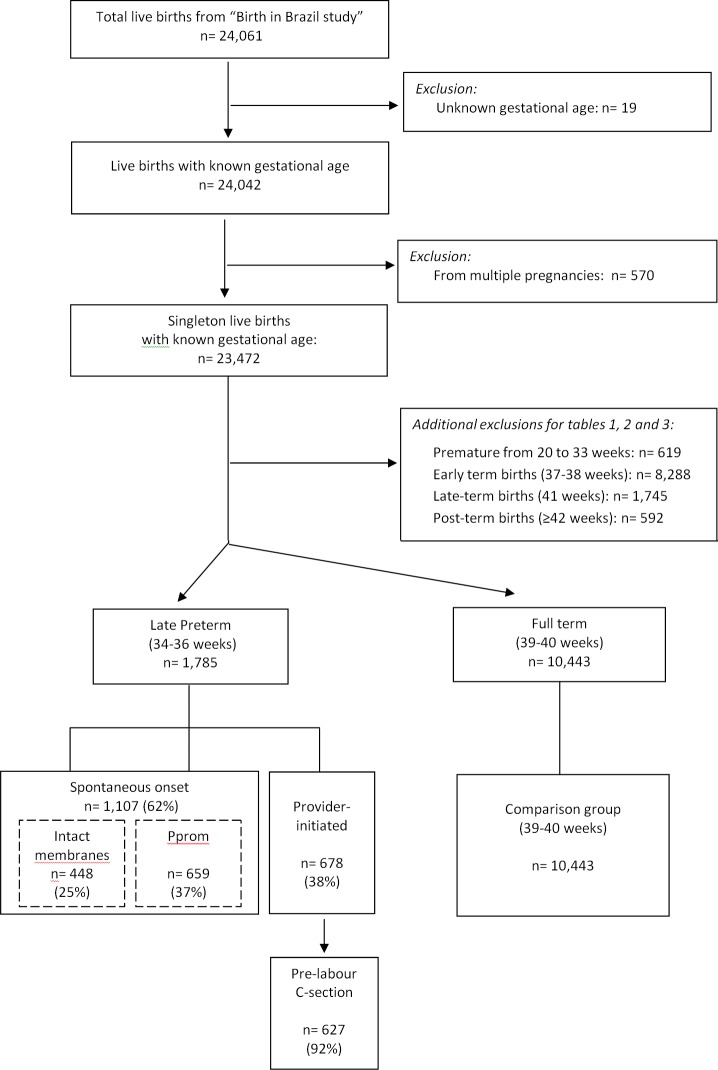
This is a sub-analysis of a national population-based survey of postpartum women entitled "Birth in Brazil", performed between 2011 and 2012. We included 23,472 singleton live births. We performed non-conditional multiple logistic regressions assessing associated factors and analysing differences between public and private health services.
Provider-initiated births accounted for 38% of late preterm births; 32% in public health services and 61% in private health services. They were associated with previous preterm birth(s) and maternal pathologies for women receiving both public and private services and with maternal age ≥35 years for women receiving public services. Women receiving private health services had higher rates of provider-initiated late preterm birth (rate of 4.8%) when compared to the ones receiving public services (rate of 2.4%), regardless of obstetric risk-adjusted OR of 2.3 (CI 1.5-3.6) for women of low obstetric risk and adjusted OR of 1.6 (CI 1.1-2.3) for women of high obstetric risk.
The high rates of provider-initiated late preterm birth suggests a considerable potential for reduction, as such prematurity can be avoided, especially in women of low obstetric risk. To promote healthy births, we advise introducing policies with incentives for the adoption of new models of birth care.
全球早产率上升的很大一部分归因于晚期早产,这可能是由于产科干预措施的增加,尤其是临产前剖宫产。晚期早产与整体早产存在相似风险,这一趋势令人担忧。在本研究中,我们描述了与医疗服务提供者发起的晚期早产相关的因素,并根据产科风险验证了公共和私立医疗服务中医疗服务提供者发起的晚期早产率的差异。
这是一项对2011年至2012年期间进行的名为“巴西出生”的全国性产后妇女人群调查的子分析。我们纳入了23472例单胎活产。我们进行了非条件多因素logistic回归分析,评估相关因素并分析公共和私立医疗服务之间的差异。
医疗服务提供者发起的分娩占晚期早产的38%;公共卫生服务中占32%,私立卫生服务中占61%。对于接受公共和私立服务的女性,它们与既往早产和母体疾病相关,对于接受公共服务的女性,它们与母亲年龄≥35岁相关。接受私立卫生服务的女性医疗服务提供者发起的晚期早产率(4.8%)高于接受公共服务的女性(2.4%),无论产科风险如何调整,低产科风险女性的调整后OR为2.3(CI 1.5 - 3.6),高产科风险女性的调整后OR为1.6(CI 1.1 - 2.3)。
医疗服务提供者发起的晚期早产率较高表明有相当大的降低潜力,因为这种早产是可以避免的,尤其是在产科风险较低的女性中。为促进健康分娩,我们建议出台政策,鼓励采用新的分娩护理模式。