Division of Research, Kaiser Permanente Oakland, California.
Dana Farber Cancer Institute, Boston, Massachusetts.
JAMA Oncol. 2016 Sep 1;2(9):1137-45. doi: 10.1001/jamaoncol.2016.0732.
Physicians and investigators have sought to determine the relationship between body mass index (BMI [calculated as weight in kilograms divided by height in meters squared]) and colorectal cancer (CRC) outcomes, but methodologic limitations including sampling selection bias, reverse causality, and collider bias have prevented the ability to draw definitive conclusions.
To evaluate the association of BMI at the time of, and following, colorectal cancer (CRC) diagnosis with mortality in a complete population using causal diagrams.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective observational study with prospectively collected data included a cohort of 3408 men and women, ages 18 to 80 years, from the Kaiser Permanente Northern California population, who were diagnosed with stage I to III CRC between 2006 and 2011 and who also had surgery.
Body mass index at diagnosis and 15 months following diagnosis.
Hazard ratios (HRs) for all-cause mortality and CRC-specific mortality compared with normal-weight patients, adjusted for sociodemographics, disease severity, treatment, and prediagnosis BMI.
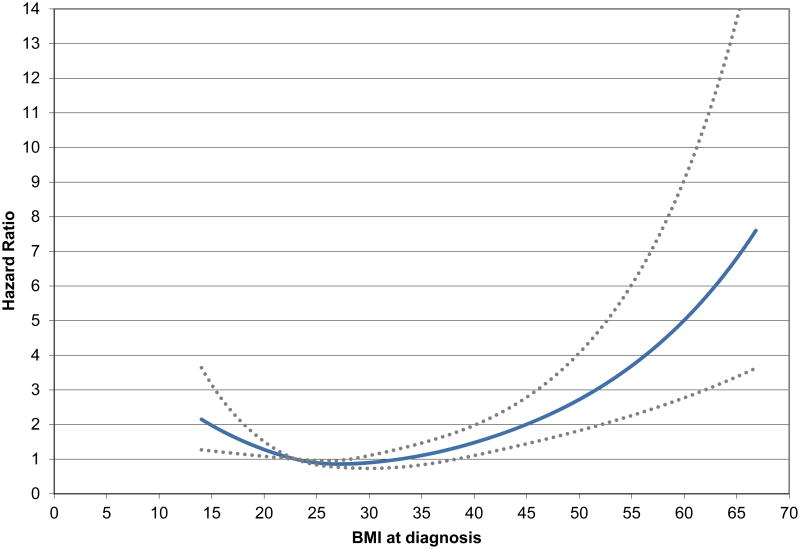
This study investigated a cohort of 3408 men and women ages 18 to 80 years diagnosed with stage I to III CRC between 2006 and 2011 who also had surgery. At-diagnosis BMI was associated with all-cause mortality in a nonlinear fashion, with patients who were underweight (BMI <18.5; HR, 2.65; 95% CI, 1.63-4.31) and patients who were class II or III obese (BMI ≥35; HR, 1.33; 95% CI, 0.89-1.98) exhibiting elevated mortality risks, compared with patients who were low-normal weight (BMI 18.5 to <23). In contrast, patients who were high-normal weight (BMI 23 to <25; HR, 0.77; 95% CI, 0.56-1.06), low-overweight (BMI 25 to <28; HR, 0.75; 95% CI, 0.55-1.04), and high-overweight (BMI 28 to <30; HR, 0.52; 95% CI, 0.35-0.77) had lower mortality risks, and patients who were class I obese (BMI 30 to <35) showed no difference in risk. Spline analysis confirmed a U-shaped relationship in participants with lowest mortality at a BMI of 28. Associations with CRC-specific mortality were similar. Associations of postdiagnosis BMI and mortality were also similar, but patients who were class I obese had significantly lower all-cause and cancer-specific mortality risks.
In this study, body mass index at the time of diagnosis and following diagnosis of CRC was associated with mortality risk. Though evidence shows that exercise in patients with cancer should be encouraged, findings suggest that recommendations for weight loss in the immediate postdiagnosis period among patients with CRC who are overweight may be unwarranted.
医生和研究人员一直在探索体重指数(BMI,体重以千克为单位除以身高以米为单位的平方)与结直肠癌(CRC)结局之间的关系,但方法学上的局限性,包括抽样选择偏倚、反向因果关系和碰撞器偏倚,使得我们无法得出明确的结论。
使用因果图评估结直肠癌(CRC)诊断时和诊断后 BMI 与死亡率之间的关联。
设计、设置和参与者:这是一项回顾性观察性研究,使用前瞻性收集的数据,纳入了 3408 名年龄在 18 至 80 岁之间的男性和女性,他们来自 Kaiser Permanente 北加利福尼亚人群,在 2006 年至 2011 年间被诊断为 I 期至 III 期 CRC,并接受了手术。
诊断时和诊断后 15 个月的体重指数。
与正常体重患者相比,所有原因死亡率和 CRC 特异性死亡率的风险比(HRs),调整了社会人口统计学、疾病严重程度、治疗和诊断前 BMI。
本研究调查了 3408 名年龄在 18 至 80 岁之间的男性和女性,他们在 2006 年至 2011 年间被诊断为 I 期至 III 期 CRC 并接受了手术。诊断时的 BMI 与全因死亡率呈非线性关联,体重不足(BMI<18.5;HR,2.65;95%CI,1.63-4.31)和 II 或 III 级肥胖(BMI≥35;HR,1.33;95%CI,0.89-1.98)的患者死亡率风险升高,与低正常体重(BMI 18.5 至<23)的患者相比。相比之下,体重正常偏高(BMI 23 至<25;HR,0.77;95%CI,0.56-1.06)、低超重(BMI 25 至<28;HR,0.75;95%CI,0.55-1.04)和高超重(BMI 28 至<30;HR,0.52;95%CI,0.35-0.77)的患者死亡率风险较低,而 BMI 30 至<35 级别的 I 级肥胖患者的死亡率风险没有差异。样条分析证实了参与者的 BMI 在 28 时死亡率最低呈 U 型关系。与 CRC 特异性死亡率的相关性相似。诊断后 BMI 和死亡率的相关性也相似,但 I 级肥胖患者的全因和癌症特异性死亡率风险显著降低。
在这项研究中,诊断时和诊断后结直肠癌的 BMI 与死亡率风险相关。尽管有证据表明应鼓励癌症患者进行运动,但研究结果表明,对于超重的 CRC 患者,在诊断后立即建议减肥可能是不必要的。