Hattori Natsuki, Hirose Yuichi, Sasaki Hikaru, Nakae Shunsuke, Hayashi Saeko, Ohba Shigeo, Adachi Kazuhide, Hayashi Takuro, Nishiyama Yuya, Hasegawa Mitsuhiro, Abe Masato
Department of Neurosurgery, Fujita Health University, Toyoake, Japan.
Department of Neurosurgery, Keio University School of Medicine, Tokyo, Japan.
Cancer Sci. 2016 Aug;107(8):1159-64. doi: 10.1111/cas.12969. Epub 2016 Jun 22.
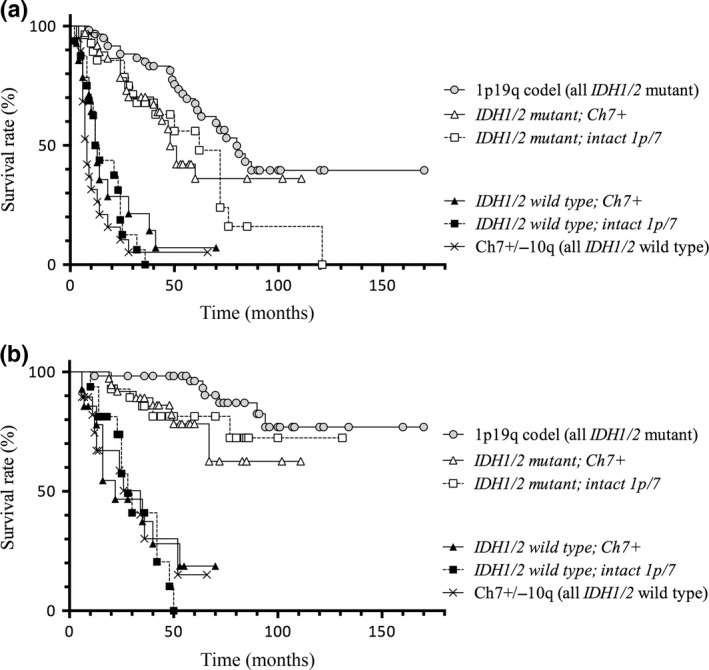
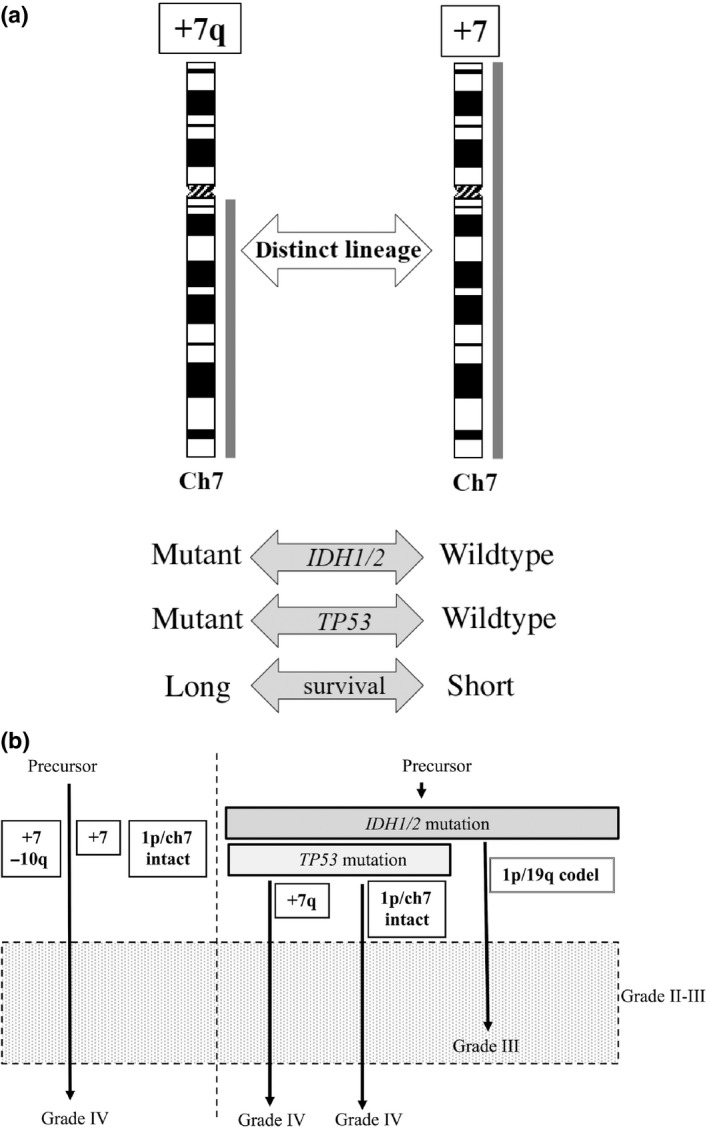
Recent investigations revealed genetic analysis provides important information in management of gliomas, and we previously reported grade II-III gliomas could be classified into clinically relevant subgroups based on the DNA copy number aberrations (CNAs). To develop more precise genetic subgrouping, we investigated the correlation between CNAs and mutational status of the gene encoding isocitrate dehydrogenase (IDH) of those tumors. We analyzed the IDH status and CNAs of 174 adult supratentorial gliomas of astrocytic or oligodendroglial origin by PCR-based direct sequencing and comparative genomic hybridization, respectively. We analyzed the relationship between genetic subclassification and clinical features. We found the most frequent aberrations in IDH mutant tumors were the combined whole arm-loss of 1p and 19q (1p/19q codeletion) followed by gain on chromosome arm 7q (+7q). The gain of whole chromosome 7 (+7) and loss of 10q (-10q) were detected in IDH wild-type tumors. Kaplan-Meier estimates for progression-free survival showed that the tumors with mutant IDH, -1p/19q, or +7q (in the absence of +7p) survived longer than tumors with wild-type IDH, +7, or -10q. As tumors with +7 (IDH wild-type) showed a more aggressive clinical nature, they are probably not a subtype that developed from the slowly progressive tumors with +7q (IDH mutant). Thus, tumors with a gain on chromosome 7 (mostly astrocytic) comprise multiple lineages, and such differences in their biological nature should be taken into consideration during their clinical management.
近期研究表明,基因分析在胶质瘤的治疗中能提供重要信息,并且我们之前报道过,基于DNA拷贝数畸变(CNA),II-III级胶质瘤可被分为具有临床相关性的亚组。为了进行更精确的基因亚组分类,我们研究了这些肿瘤中CNA与异柠檬酸脱氢酶(IDH)编码基因突变状态之间的相关性。我们分别通过基于聚合酶链反应(PCR)的直接测序和比较基因组杂交技术,分析了174例成人幕上星形细胞或少突胶质细胞起源的胶质瘤的IDH状态和CNA。我们分析了基因亚分类与临床特征之间的关系。我们发现,IDH突变型肿瘤中最常见的畸变是1p和19q的全臂联合缺失(1p/19q共缺失),其次是7号染色体臂的增益(+7q)。在IDH野生型肿瘤中检测到了7号染色体的增益(+7)和10号染色体的缺失(-10q)。无进展生存期的Kaplan-Meier估计显示,具有IDH突变、-1p/19q或+7q(无+7p)的肿瘤比具有野生型IDH、+7或-10q的肿瘤存活时间更长。由于具有+7(IDH野生型)的肿瘤表现出更具侵袭性的临床特性,它们可能不是由具有+7q(IDH突变)的缓慢进展性肿瘤发展而来的亚型。因此,具有7号染色体增益的肿瘤(大多为星形细胞性)包含多个谱系,在其临床治疗过程中应考虑到它们生物学特性的这种差异。