Lee Yi-Chien, Hsiao Chih-Yen, Hung Miao-Chiu, Hung Sheng-Che, Wang Hung-Ping, Huang Yun-Jhong, Wang Jann-Tay
From the Department of Internal Medicine (Y-CL, C-YH, H-PW), Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chia-Yi; Department of Hospital and Health Care Administration (C-YH), Chia Nan University of Pharmacy and Science, Tainan; Department of Pediatrics (M-CH); Department of Radiology (S-CH), Taipei Veterans General Hospital; School of Medicine (S-CH), National Yang-Ming University, Taipei; Department of Colorectal Surgery (Y-JH), Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chia-Yi; and Department of Internal Medicine (J-TW), National Taiwan University Hospital, Taipei, Taiwan.
Medicine (Baltimore). 2016 May;95(20):e3694. doi: 10.1097/MD.0000000000003694.
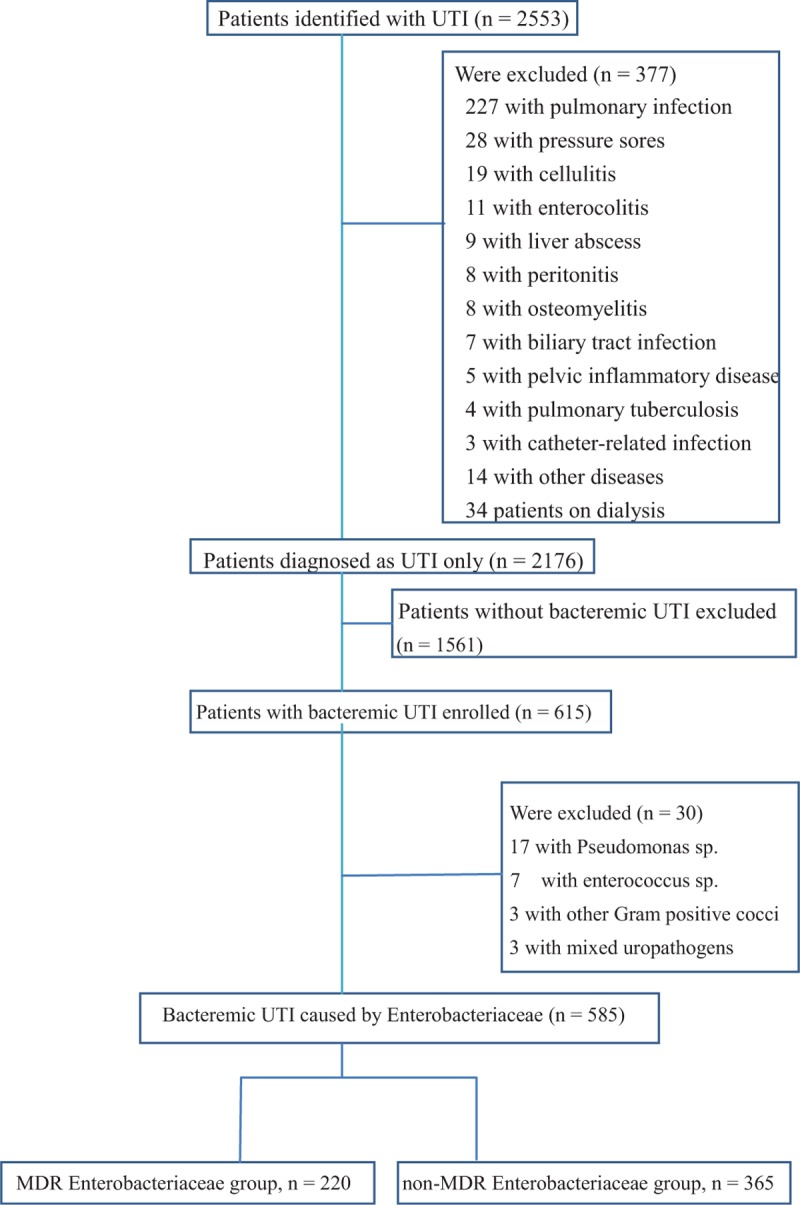
The purpose of this study is to compare the clinical features and treatment outcomes among patients with bacteremic urinary tract infection (UTI) caused by multidrug-resistant (MDR) and non-MDR Enterobacteriaceae and to identify whether MDR pathogens were independently associated with severe sepsis or septic shock at presentation.The clinical data of adult patients visiting and being treated at Chia-Yi Christian Hospital due to bacteremic UTI caused by Enterobacteriaceae from January 2006 to August 2015 were retrospectively analyzed.A total of 585 patients were enrolled. Among them, 220 (37.6%) were caused by the MDR Enterobacteriaceae. A total of 206 patients (35.2%) developed severe sepsis or septic shock at presentation. Patients in the MDR group tend to be male and have a past history of gout, recurrent UTI, prior hospitalization, hydronephrosis, renal stone, ureteral stone, indwelling urinary catheter, newly development of renal dysfunction, severe sepsis or septic shock, intensive care unit (ICU) admission, receipt of ineffective empirical therapy, longer hospital stay, and higher in-hospital mortality (2.7% vs 1.9%, P = 0.569). Using multivariate logistic regression analysis, it is revealed that independent predictors associated with severe sepsis or septic shock at presentation were liver cirrhosis (OR 2.868; 95% CI 1.439-5.716; P = 0.003), indwelling urinary catheter (OR 1.936; 95% CI 1.238-3.027; P = 0.004), and MDR Enterobacteriaceae (OR 1.447; 95% CI 1.002-2.090; P = 0.049).Multidrug resistance was associated with the development of severe sepsis or septic shock upon presentation among patients with bacteremic UTI caused by Enterobacteriaceae. Therefore, empirical antibiotics therapy for patients with UTI presented with severe sepsis and/or septic shock should be more broad-spectrum to effectively cover MDR Enterobacteriaceae.
本研究旨在比较由多重耐药(MDR)和非MDR肠杆菌科细菌引起的菌血症性尿路感染(UTI)患者的临床特征和治疗结果,并确定MDR病原体在就诊时是否与严重脓毒症或感染性休克独立相关。对2006年1月至2015年8月因肠杆菌科细菌引起的菌血症性UTI在嘉义基督教医院就诊并接受治疗的成年患者的临床资料进行回顾性分析。共纳入585例患者。其中,220例(37.6%)由MDR肠杆菌科细菌引起。共有206例患者(35.2%)在就诊时发生严重脓毒症或感染性休克。MDR组患者倾向于男性,并有痛风、复发性UTI、既往住院、肾积水、肾结石、输尿管结石、留置导尿管、新出现的肾功能不全、严重脓毒症或感染性休克、入住重症监护病房(ICU)、接受无效的经验性治疗、住院时间更长以及院内死亡率更高(2.7%对1.9%,P = 0.569)。使用多因素逻辑回归分析显示,与就诊时严重脓毒症或感染性休克相关的独立预测因素为肝硬化(比值比[OR]2.868;95%置信区间[CI]1.439 - 5.716;P = 0.003)、留置导尿管(OR 1.936;95% CI 1.238 - 3.027;P = 0.004)和MDR肠杆菌科细菌(OR 1.447;95% CI 1.002 - 2.090;P = 0.049)。多重耐药与肠杆菌科细菌引起的菌血症性UTI患者就诊时严重脓毒症或感染性休克的发生相关。因此,对于出现严重脓毒症和/或感染性休克的UTI患者,经验性抗生素治疗应更具广谱性,以有效覆盖MDR肠杆菌科细菌。