Van Dyke Russell B, Chadwick Ellen Gould, Hazra Rohan, Williams Paige L, Seage George R
Department of Pediatrics, Tulane University School of Medicine , New Orleans, LA , USA.
Department of Pediatrics, Feinberg School of Medicine, Northwestern University (NUFSM) , Chicago, IL , USA.
Front Immunol. 2016 May 23;7:199. doi: 10.3389/fimmu.2016.00199. eCollection 2016.
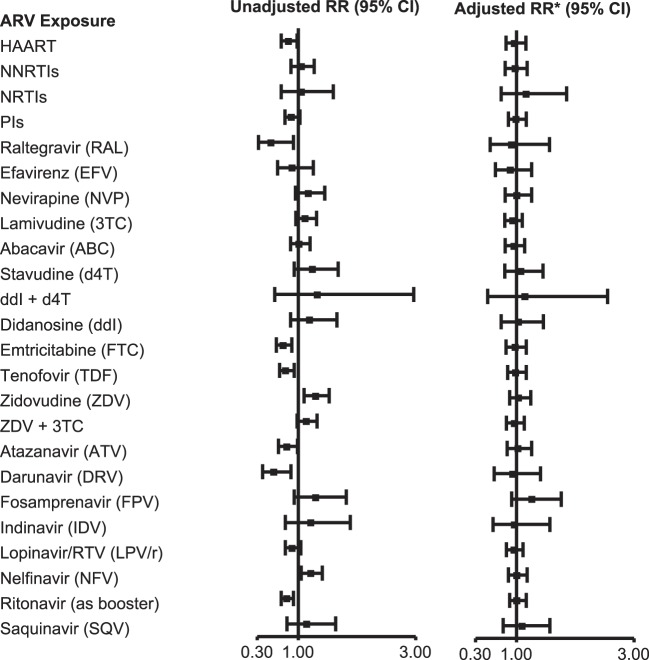
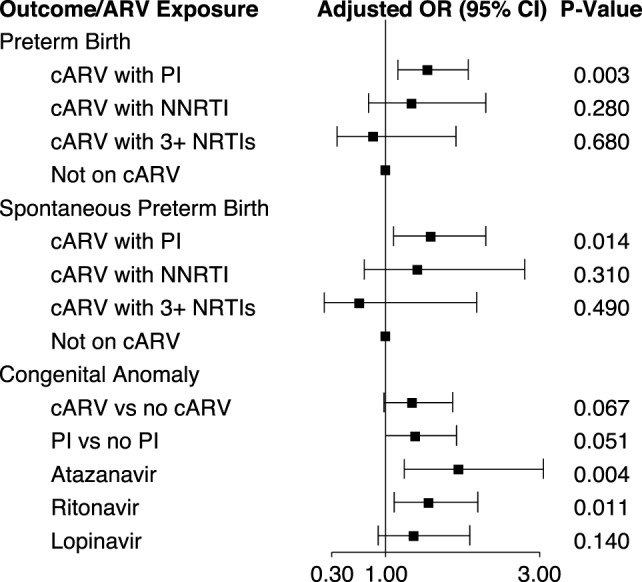
The Surveillance Monitoring for ART Toxicities (SMARTT) cohort of the Pediatric HIV/AIDS Cohort Study includes over 3,500 HIV-exposed but uninfected infants and children at 22 sites in the US, including Puerto Rico. The goal of the study is to determine the safety of in utero exposure to antiretrovirals (ARVs) and to estimate the incidence of adverse events. Domains being assessed include metabolic, growth and development, cardiac, neurological, neurodevelopmental (ND), behavior, language, and hearing. SMARTT employs an innovative trigger-based design as an efficient means to identify and evaluate adverse events. Participants who met a predefined clinical or laboratory threshold (trigger) undergo additional evaluations to define their case status. After adjusting for birth cohort and other factors, there was no significant increase in the likelihood of meeting overall case status (case in any domain) with exposure to combination ARVs (cARVs), any ARV class, or any specific ARV. However, several individual ARVs were significantly associated with case status in individual domains, including zidovudine for a metabolic case, first trimester stavudine for a language case, and didanosine plus stavudine for a ND case. We found an increased rate of preterm birth with first trimester exposure to protease inhibitor-based cARV. Although there was no overall increase in congenital anomalies with first trimester cARV, a significant increase was seen with exposure to atazanavir, ritonavir, and didanosine plus stavudine. Tenofovir exposure was associated with significantly lower mean whole-body bone mineral content in the newborn period and a lower length and head circumference at 1 year of age. With ND testing at 1 year of age, specific ARVs (atazanavir, ritonavir-boosted lopinavir, nelfinavir, and tenofovir) were associated with lower performance, although all groups were within the normal range. No ARVs or classes were associated with lower performance between 5 and 13 years of age. Atazanavir and saquinavir exposure were associated with late language emergence at 1 year, but not at 2 years of age. The results of the SMARTT study are generally reassuring, with little evidence for serious adverse events resulting from in utero ARV exposure. However, several findings of concern warrant further evaluation, and new ARVs used in pregnancy need to be evaluated.
儿科艾滋病毒/艾滋病队列研究的抗逆转录病毒疗法毒性监测(SMARTT)队列包括美国22个地点(包括波多黎各)的3500多名暴露于艾滋病毒但未感染的婴儿和儿童。该研究的目的是确定子宫内暴露于抗逆转录病毒药物(ARV)的安全性,并估计不良事件的发生率。正在评估的领域包括代谢、生长发育、心脏、神经、神经发育(ND)、行为、语言和听力。SMARTT采用了一种创新的基于触发因素的设计,作为识别和评估不良事件的有效手段。达到预定义临床或实验室阈值(触发因素)的参与者要接受额外评估,以确定其病例状态。在对出生队列和其他因素进行调整后,暴露于联合抗逆转录病毒药物(cARV)、任何抗逆转录病毒药物类别或任何特定抗逆转录病毒药物的情况下,达到总体病例状态(任何领域的病例)的可能性没有显著增加。然而,几种个别抗逆转录病毒药物与个别领域的病例状态显著相关,包括齐多夫定与代谢病例、孕早期司他夫定与语言病例、去羟肌苷加司他夫定与神经发育病例。我们发现孕早期暴露于基于蛋白酶抑制剂的cARV会导致早产率增加。虽然孕早期cARV暴露导致的先天性异常总体上没有增加,但暴露于阿扎那韦、利托那韦以及去羟肌苷加司他夫定会导致显著增加。替诺福韦暴露与新生儿期平均全身骨矿物质含量显著降低以及1岁时身长和头围较低有关。在1岁时进行神经发育测试时,特定的抗逆转录病毒药物(阿扎那韦、利托那韦增强的洛匹那韦、奈非那韦和替诺福韦)与较低的表现有关,尽管所有组都在正常范围内。在5至13岁之间,没有抗逆转录病毒药物或药物类别与较低的表现有关。阿扎那韦和沙奎那韦暴露与1岁时语言发育延迟有关,但2岁时没有。SMARTT研究的结果总体上令人放心,几乎没有证据表明子宫内抗逆转录病毒药物暴露会导致严重不良事件。然而,一些令人担忧的发现值得进一步评估,并且需要对孕期使用的新型抗逆转录病毒药物进行评估。