Heo Yang Hoi, Yagi Shunjiro, Toriyama Kazuhiro, Takanari Keisuke, Fujimoto Yasushi, Nishio Naoki, Fujii Masazumi, Saito Kiyoshi, Takahashi Masakatsu, Kamei Yuzuru
Department of Plastic and Reconstructive Surgery, Nagoya University Graduate School of Medicine, Nagoya, Aichi, Japan; Department of Plastic and Reconstructive Surgery, Tottori University Faculty of Medicine, Yonago, Tottori, Japan; Department of Plastic and Reconstructive Surgery, Nagoya City University Hospital, Nagoya, Aichi, Japan; Department of Otorhinolaryngology, Nagoya University Graduate School of Medicine, Nagoya, Aichi, Japan; Department of Neurosurgery, Fukushima Medical University, Fukushima, Fukushima, Japan; and Department of Otorhinolaryngology, Kariya Toyota General Hospital, Kariya, Aichi, Japan.
Plast Reconstr Surg Glob Open. 2016 Mar 8;4(3):e636. doi: 10.1097/GOX.0000000000000645. eCollection 2016 Mar.
Although we have seen tremendous advancement in microsurgery over the last 2 decades and free tissue transfer has become standard for head and neck reconstruction, surgeons still struggle to prevent postoperative complications. We examined the relationship between body mass index (BMI) and postoperative complications in patients undergoing rectus abdominis free flap transfer after anterolateral craniofacial resection.
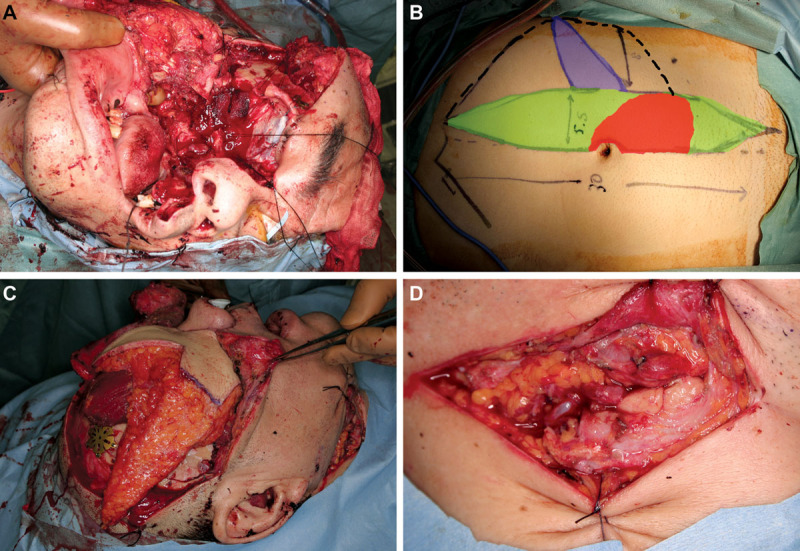
This was a retrospective review of reconstructive surgery using rectus abdominis musculocutaneous free flap in patients with locally advanced maxillary sinus carcinoma from 2003 to 2014 (n = 35, 27 men and 8 women; average age, 60.9 ± 7.8 years). All patients underwent craniofacial reconstruction after anterior and middle cranial fossa skull base resection and maxillectomy (class IV, subtype a) with palatal resection. Patients were categorized based on sex, BMI, and other parameters.
Recipient-site infection occurred in 11 patients (31.4%), cerebrospinal fluid leakage in 6 (17.1%), partial flap necrosis in 2 (5.7%), total flap necrosis in 1 (2.9%), and facial fistula in 4 (11.4%). Women showed partial flap necrosis significantly more frequently (P = 0.047), probably owing to poor vascular supply of the subcutaneous fat layer. Patients with low BMI (<20 kg/m(2)) showed recipient-site infection (P = 0.02) and facial fistula (P = 0.01) significantly more frequently owing to insufficient tissue volume and poor vascular supply.
Postoperative recipient-site infection and facial fistula occurred mainly in low-BMI patients. Surgeons should take care to achieve sufficient donor tissue on low-BMI patients. Using a prosthetic obturator in low-BMI patients for craniofacial reconstruction can be a good alternative option to reduce postoperative complications due to insufficient donor tissue volume.
尽管在过去20年里我们见证了显微外科手术的巨大进步,游离组织移植已成为头颈部重建的标准方法,但外科医生仍在努力预防术后并发症。我们研究了前外侧颅面切除术后接受腹直肌游离皮瓣移植患者的体重指数(BMI)与术后并发症之间的关系。
这是一项对2003年至2014年局部晚期上颌窦癌患者使用腹直肌肌皮游离皮瓣进行重建手术的回顾性研究(n = 35,27名男性和8名女性;平均年龄60.9±7.8岁)。所有患者在颅前窝和颅中窝颅底切除及上颌骨切除(IV类,a亚型)并进行腭切除术后接受颅面重建。患者根据性别、BMI和其他参数进行分类。
11例患者(31.4%)发生受区感染,6例(17.1%)发生脑脊液漏,2例(5.7%)发生部分皮瓣坏死,1例(2.9%)发生全皮瓣坏死,4例(11.4%)发生面部瘘管。女性发生部分皮瓣坏死的频率明显更高(P = 0.047),可能是由于皮下脂肪层血供较差。低BMI(<20 kg/m²)患者因组织量不足和血供较差,受区感染(P = 0.02)和面部瘘管(P = 0.01)的发生率明显更高。
术后受区感染和面部瘘管主要发生在低BMI患者中。外科医生应注意为低BMI患者获取足够的供区组织。对于低BMI患者,在颅面重建中使用修复性闭孔器可能是减少因供区组织量不足导致术后并发症的一个良好替代选择。