Hart Allyson, Salkowski Nicholas, Snyder Jon J, Israni Ajay K, Kasiske Bertram L
1 Department of Medicine, Hennepin County Medical Center, University of Minnesota, Minneapolis, MN. 2 Scientific Registry of Transplant Recipients, Minneapolis Medical Research Foundation, Minneapolis, MN. 3 Division of Epidemiology and Community Health, School of Public Health, University of Minnesota, Minneapolis, MN.
Transplantation. 2016 Jul;100(7):1564-70. doi: 10.1097/TP.0000000000001185.
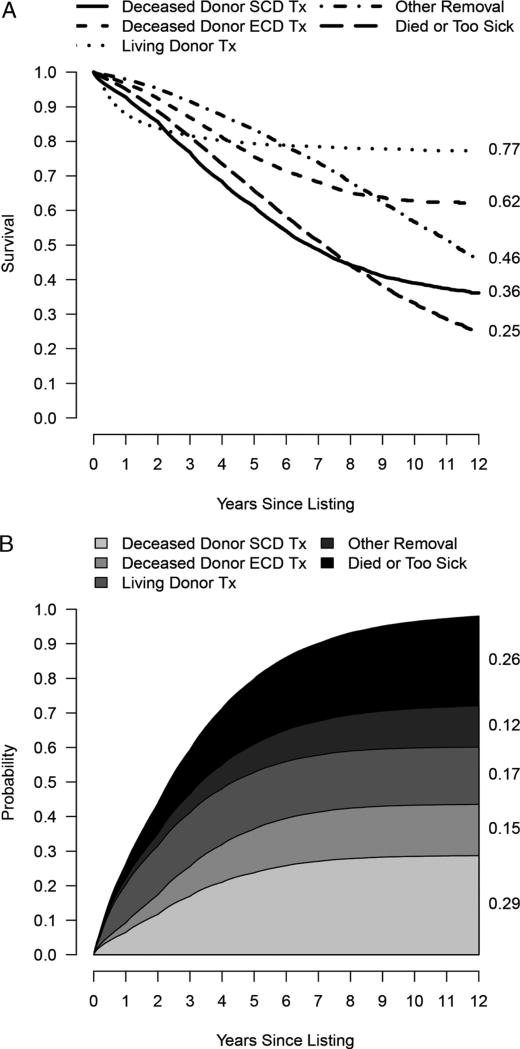
Median historical time to kidney transplant is misleading because it does not convey the competing risks of death or removal from the waiting list. We developed and validated a competing risk model to calculate likelihood of outcomes for kidney transplant candidates and demonstrate how this information differs from median time to transplant.
Data were obtained from the US Scientific Registry of Transplant Recipients. The retrospective cohort included 163 636 adults listed for kidney transplant before December 31, 2011. Predictors were age, sex, blood type, calculated panel-reactive antibodies, donation service area, dialysis duration, comorbid conditions, and body mass index. Outcomes were deceased or living donor transplant, death or removal from the list due to deteriorating medical condition, or removal due to other reasons. We calculated hazards for the possible outcomes, then the cumulative incidence function for a given candidate using competing risk methodology. Discrimination and calibration were assessed through C statistics and calibration plots for each cause-specific Cox proportional hazard model.
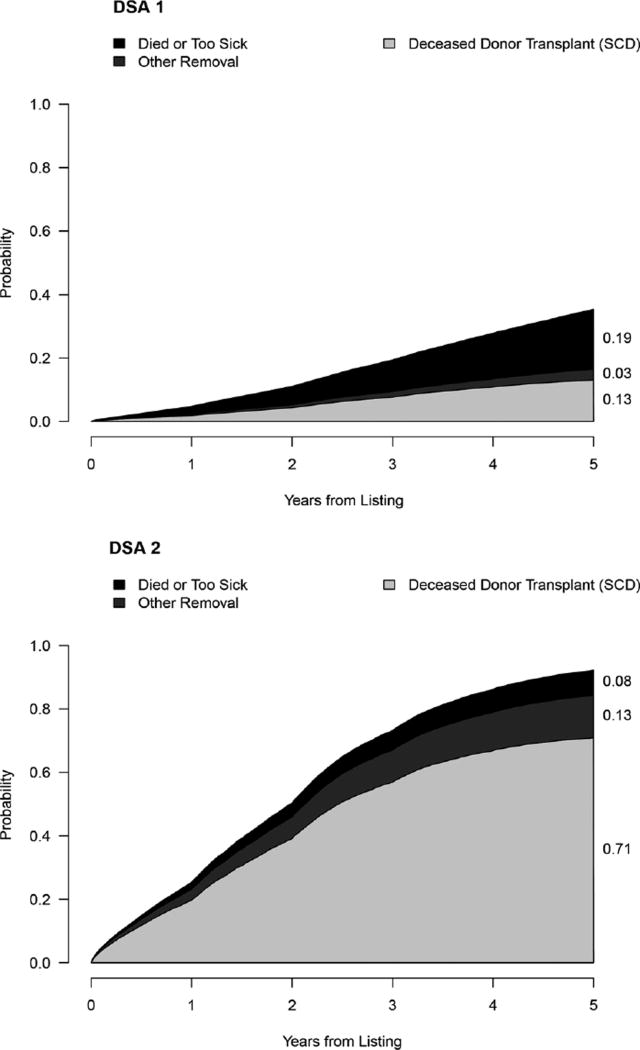
C statistics ranged from 0.64 to 0.73. Calibration plots showed good calibration. The competing risk model shows probability of all possible outcomes for up to 12 years given a candidate's characteristics, contrasted with the median waiting time for that candidate's donation service area.
A competing risk model conveys more relevant information than the median waiting time for a given transplant center. This model will be updated to create a calculator reflecting the most recent outcomes and changes in allocation policy. It illustrates the conversations that should be initiated with transplant candidates.
既往肾移植的中位时间具有误导性,因为它没有体现死亡或从等待名单中移除的竞争风险。我们开发并验证了一种竞争风险模型,以计算肾移植候选者的预后可能性,并展示该信息与移植中位时间的差异。
数据来自美国移植受者科学登记处。回顾性队列包括2011年12月31日前登记等待肾移植的163636名成年人。预测因素包括年龄、性别、血型、计算得出的群体反应性抗体、捐赠服务区、透析时间、合并症和体重指数。结局包括 deceased 或活体供者移植、因病情恶化死亡或从名单中移除,或因其他原因移除。我们计算了可能结局的风险,然后使用竞争风险方法计算给定候选者的累积发病率函数。通过每个特定原因的Cox比例风险模型的C统计量和校准图评估区分度和校准情况。
C统计量范围为0.64至0.73。校准图显示校准良好。竞争风险模型显示了根据候选者特征在长达12年内所有可能结局的概率,与该候选者捐赠服务区的中位等待时间形成对比。
竞争风险模型比给定移植中心的中位等待时间传达了更相关的信息。该模型将更新以创建一个反映最新结局和分配政策变化的计算器。它说明了应该与移植候选者展开的对话。 (注:“deceased”此处可能是文档录入有误,推测可能是“deceased donor transplant”即“ deceased供者移植”,但按要求未做修改)