Rey Jacques, Poitiers Franck, Paehler Tobias, Brunet Aurélie, DiCioccio A Thomas, Cannon Christopher P, Surks Howard K, Pinquier Jean-Louis, Hanotin Corinne, Sasiela William J
Sanofi, Paris, France.
Sanofi, Paris, France
J Am Heart Assoc. 2016 Jun 10;5(6):e003323. doi: 10.1161/JAHA.116.003323.
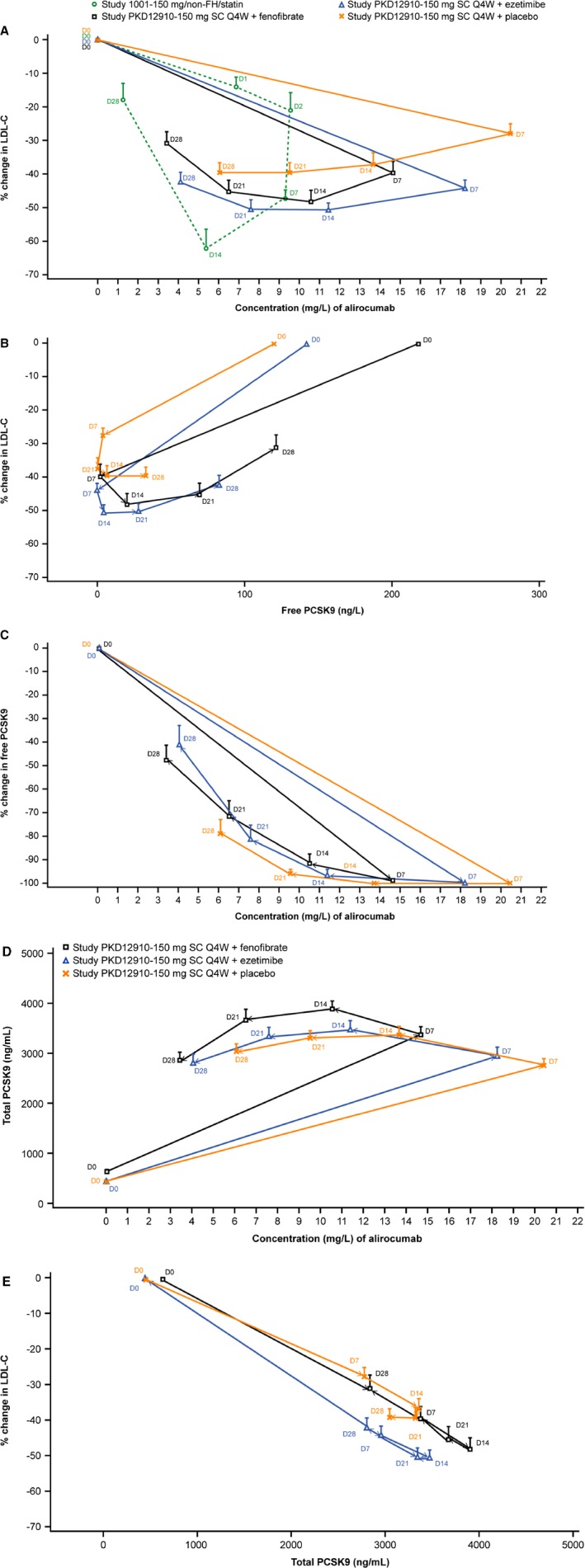
Alirocumab undergoes target-mediated clearance via binding of proprotein convertase subtilisin/kexin type 9 (PCSK9). Statins increase PCSK9 levels; the effects of nonstatin lipid-lowering therapies are unclear. Every-4-weeks dosing of alirocumab may be appropriate for some patients in absence of background statin but is not yet approved.
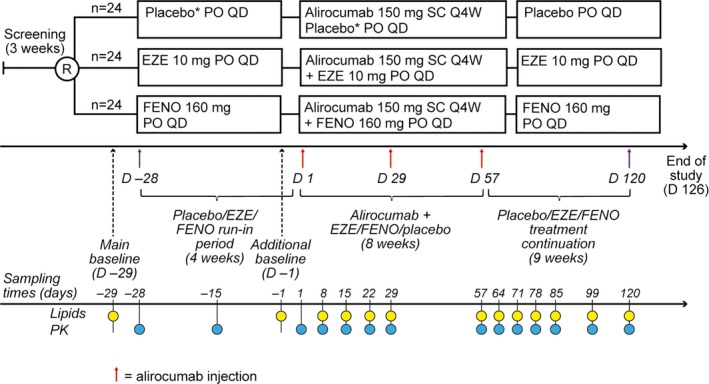
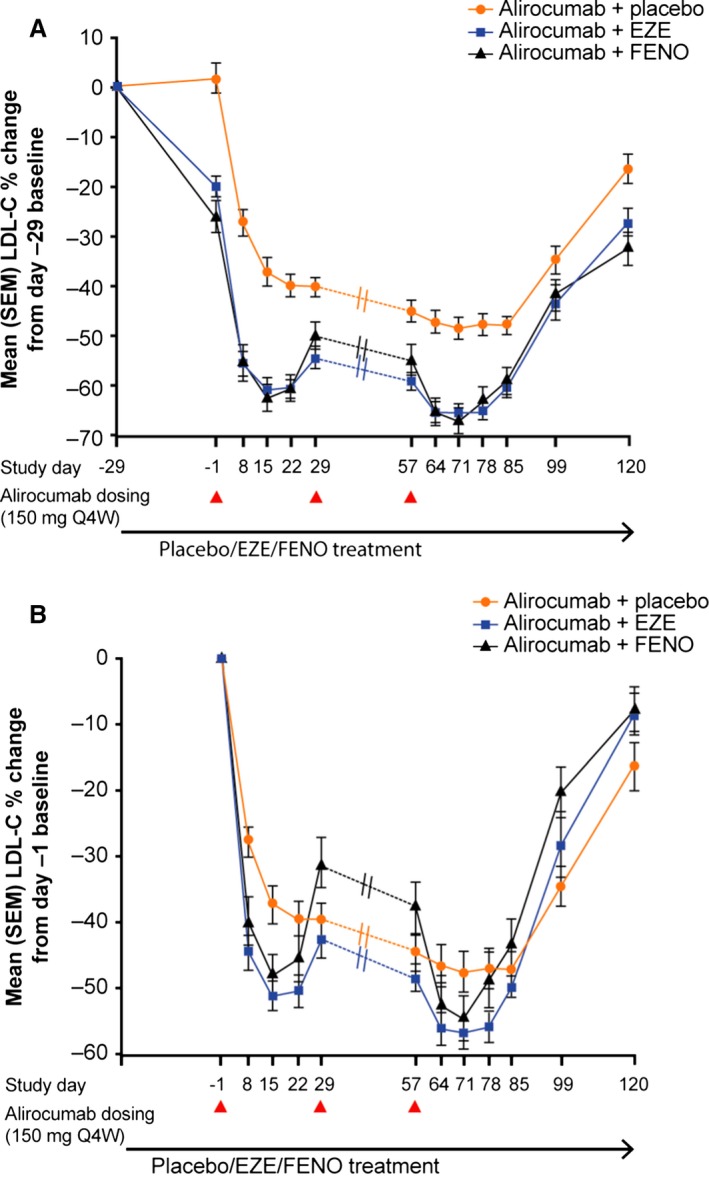
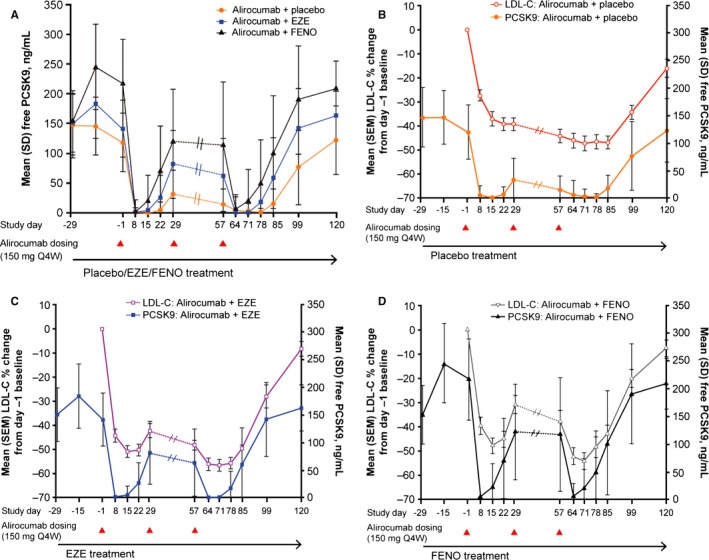
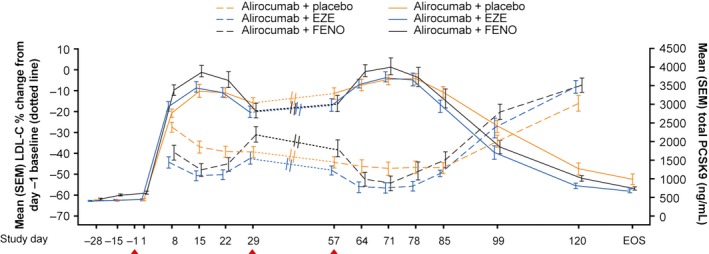
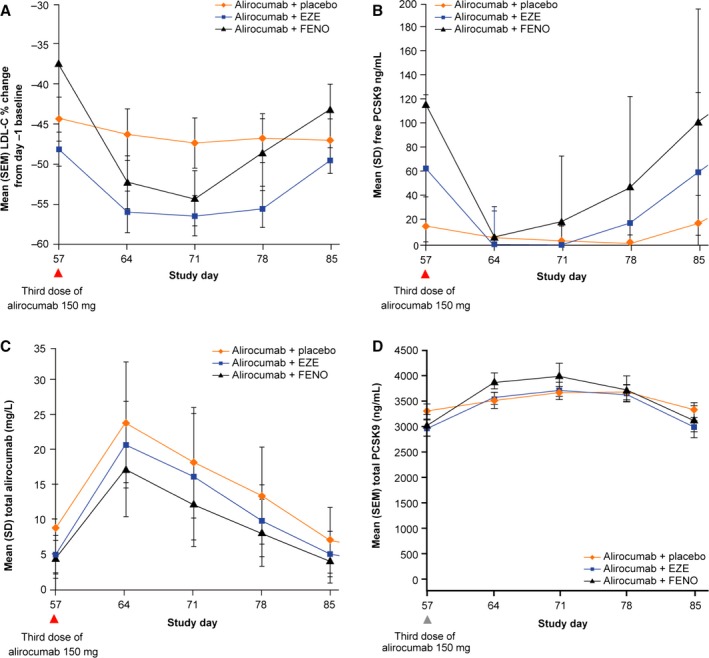
Low-density lipoprotein cholesterol (LDL-C), PCSK9, and alirocumab levels were assessed in subjects (LDL-C >130 mg/dL, n=24/group) after a 4-week run-in taking oral ezetimibe, fenofibrate, or ezetimibe placebo, when alirocumab 150 mg every 4 weeks (days 1, 29, and 57) was added. Maximal mean LDL-C reductions from day -1 baseline (prealirocumab) occurred on day 71 in all groups: alirocumab plus placebo, 47.4%; alirocumab plus ezetimibe, 56.6%; and alirocumab plus fenofibrate, 54.3%. LDL-C reductions were sustained through day 85 with alirocumab plus placebo (47.0%); the duration of effect was slightly diminished at day 85 versus day 71 with ezetimibe (49.6%) or fenofibrate combinations (43.2%). Free PCSK9 concentrations were lowest at day 71 in all groups, then increased over time; by day 85, free PCSK9 concentrations were higher, and alirocumab levels lower, with alirocumab plus fenofibrate, and to a lesser extent alirocumab plus ezetimibe, versus alirocumab plus placebo.
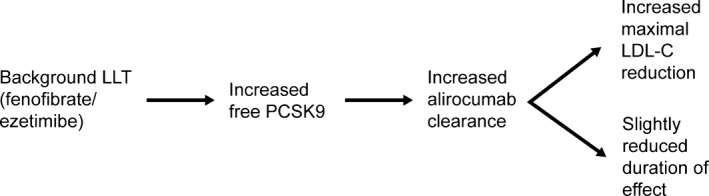
Alirocumab 150 mg every 4 weeks produced maximal LDL-C reductions of 47% in combination with placebo and 54% to 57% in combination with ezetimibe or fenofibrate. The oral lipid-lowering therapies appear to increase PCSK9 levels, leading to increased alirocumab clearance. Although the duration of effect was modestly diminished with alirocumab plus ezetimibe/fenofibrate versus placebo, the effect was less than observed in trials with background statins, and it would not preclude the use of alirocumab every 4 weeks in patients taking these nonstatin lipid-lowering therapies concomitantly.
URL: http://www.Clinicaltrials.gov. Unique identifier: NCT01723735.
阿利西尤单抗通过与前蛋白转化酶枯草溶菌素9型(PCSK9)结合进行靶点介导的清除。他汀类药物会升高PCSK9水平;非他汀类降脂疗法的效果尚不清楚。对于一些未服用背景他汀类药物的患者,每4周一次的阿利西尤单抗给药可能是合适的,但尚未获批。
在接受口服依折麦布、非诺贝特或依折麦布安慰剂4周导入期后,当每4周(第1天、第29天和第57天)添加150mg阿利西尤单抗时,对受试者(低密度脂蛋白胆固醇[LDL-C]>130mg/dL,每组n=24)的LDL-C、PCSK9和阿利西尤单抗水平进行评估。所有组从第-1天基线(阿利西尤单抗治疗前)开始的最大平均LDL-C降低出现在第71天:阿利西尤单抗加安慰剂组为47.4%;阿利西尤单抗加依折麦布组为56.6%;阿利西尤单抗加非诺贝特组为54.3%。阿利西尤单抗加安慰剂组在第85天LDL-C降低仍持续(47.0%);与依折麦布(49.6%)或非诺贝特联合用药组相比,第85天的疗效持续时间与第71天相比略有缩短(43.2%)。所有组在第71天游离PCSK9浓度最低,然后随时间增加;到第85天,与阿利西尤单抗加安慰剂组相比,阿利西尤单抗加非诺贝特组游离PCSK9浓度更高,阿利西尤单抗水平更低,阿利西尤单抗加依折麦布组的程度稍轻。
每4周一次的150mg阿利西尤单抗与安慰剂联合使用时,LDL-C最大降低47%,与依折麦布或非诺贝特联合使用时降低54%至57%。口服降脂疗法似乎会升高PCSK9水平,导致阿利西尤单抗清除增加。虽然与安慰剂相比,阿利西尤单抗加依折麦布/非诺贝特组的疗效持续时间略有缩短,但效果小于在有背景他汀类药物的试验中观察到的情况,并且这并不排除在同时服用这些非他汀类降脂疗法的患者中每4周使用一次阿利西尤单抗。